

Ⅰ. 서 론
1. 연구 배경 및 필요성
응급의료에 관한 법률에 따르면 응급환자란 즉시 필요한 응급처치를 받지 않을 경우, 생명을 보존할 수 없거나 심신상의 중대한 위해가 발생될 가능성이 있는 환자 또는 이에 준하는 자를 지칭한다[1]. 병원 전 처치는 응급환자 발생 시 환자의 생존율과 예후에 영향을 미치는 중요한 요소 중 하나이다. 병원 전 처치를 주로 담당하는 응급구조사는 응급환자 발생 현장에서 응급환자를 위해 상담, 구조 및 이송의 업무를 수행하고 있다[2]. 이처럼 응급구조사는 응급의료체계에서 응급환자의 생존과 예후에 영향을 미칠 수 있는 조치를 취하는 중요한 역할을 수행하고 있기 때문에[3], 전문성이 중요한 직군임을 알 수 있다[4].
응급의료의 경우 비교적 역사가 짧고 정보와 기술의 변화 속도가 빠르기 때문에 변화에 발맞춰 나가며 환자들에게 최선의 처치를 제공하기 위해서 적절한 보수교육이 필수적이다[5]. 이에 1995년 응급구조사 제도가 도입된 이후, 응급구조사의 전문성 유지와 역량 강화를 위해 1997년부터 1999년까지는 응급구조사 양성기관에서 보수교육을 실시하기 시작하였고, 2000년도에는 의약 분업으로 인하여 보수교육이 없었으나 이후 2001년부터는 응급구조사 양성기관과 함께 대한응급구조사협회가 응급구조사 보수교육을 시행해나가며 응급구조사의 역량 향상을 위한 노력들을 꾸준히 수행해 왔다[2]. 국내 보수교육의 교육 대상자는 응급구조사 자격증을 취득한 후 그다음 해부터 보수교육 이수 대상자가 되며, 교육 주기는 1년, 보수교육 시간은 4~8시간이 평균적이고 보수교육 주제는 해마다 유동적인 내용으로 진행이 되고 있다[6].
그러나 현재 응급구조사의 보수교육 참여율은 다른 의료 직종에 비해 낮았다[7]. 또한 국외의 응급구조사 보수교육 프로그램과 비교 했을 때 국내의 보수교육은 미국이나 일본에 비해 교육 프로그램의 질적인 측면이나 교육 시간 면에서 모두 차이가 있었으며[6, 8], 국내 보수교육 내용의 질적 개선 요구도는 높게 나타났다[7].
이는 국민 생활 수준 향상을 통해, 의료에 대한 권리 의식이 신장되었고 보건의료 서비스의 질적 향상 요구도가 증대되고 있음에도 불구하고, 양적 수준 향상에 비해 질적 수준의 향상은 미비한 것으로 보여진다[6, 9]. 따라서, 응급환자들에게 전문적인 양질의 응급의료 서비스를 제공하기 위해서 실질적이고, 효율성 있는 교육프로그램을 제공하여 보수교육의 만족도와 참여율을 높여, 전문성을 유지하고 역량을 강화해나가는 것이 중요하다[9].
이에 본 연구는 응급구조사의 질적 향상과 업무 역량 강화를 위한 보수교육의 발전 방향을 제안하고자, 체계적 문헌고찰이라는 연구방법론을 이용하여 이전까지의 응급구조사 보수교육에 관한 연구를 종합하는데 그 목적이 있다.
Ⅱ. 연구방법
1. 연구설계
이 연구는 국내·외에서 진행된 응급구조사 보수교육 관련 연구 현황을 파악하고 교육의 만족도 및 제안 사항을 파악하기 위해 시행된 체계적 문헌고찰 연구이다. 본 연구의 모든 과정은 PRISMA(Preferred reporting items for systematic reviews and meta-analyses) guidelines[10]에 준거하여 시행되었다. 논문의 객관성을 확보하기 위하여 문헌선택 흐름도(PRISMA flowchart)에 기초하여 2명의 연구자가 각각 독립적으로 문헌검색을 수행하였다. 문헌검색을 통해 추출된 문헌은 선정 기준에 따라 분류하였다. 문헌 선정과정에서 연구자 간 상이한 의견이 발생한 경우, 연구자 간 이견을 조정하여 범위 및 분류 기준을 수정하였고, 최종 선정된 모든 문헌은 비뚤림 위험평가를 실시하였다. 확정된 분석 기준은 보수교육 실태 조사, 보수교육 방법 제안, 보수교육 과목 제안이었으며 이를 중심으로 정보를 추출하여 문헌을 분석하였다.
2. 문헌 검색 및 선정
1) 문헌검색
본 연구는 2020년 12월 28일까지 웹 기반 데이터베이스에 출판된 학술지를 분석 대상으로 선정하였다. 국내 문헌은 한국학술정보(KISS), 한국연구정보서비스(RISS), 한국학술지인용색인(KCI), 국회전자도서관을 활용하였고, 국외 문헌은 Pubmed와 Embase의 데이터베이스를 사용하였다. 회색 문헌으로는 Kyobo scholar의 데이터베이스를 사용하였다. 검색어는 ‘응급구조사’ OR ‘구급대원’ AND ‘보수교육’과 ‘Emergency medical technicians’ OR ‘Paramedic’ OR ‘EMT’ AND ‘Continuing education’으로 검색하였다. 문헌 검색 시 학위 논문은 제외하고 학술 논문만으로 검색 결과를 국한하였다. 발행기관과 게재 시기에는 별도의 제한을 두지 않았다. 그 결과 국내 데이터베이스를 통해 검색된 문헌 수는 434편, 국외 데이터베이스를 활용해 검색된 문헌 수는 1,511편이었다. 회색 문헌 41편으로, 문헌 검색을 통하여 추출된 문헌의 수는 1,986편이었다. 이후, 2차 문헌 선택/배제를 진행한 후 수기 문헌 중 1편을 추가하여 최종적으로 1,987편의 문헌을 추출하였다.
2) 문헌선정
문헌 검색을 통하여 추출된 총 1,986편의 문헌 중 중복검색 된 174편을 제외한 1,812편에 대해서 문헌 선정 기준을 적용하였다. 문헌 선정 과정은 사전의 합의된 선택 및 배제기준에 근거하여 두 명의 연구자가 독립적으로 수행하였다. 1차 문헌 선택/배제 과정에서는 문헌의 제목과 초록을 통해 응급구조사 보수교육과 직접적으로 관련성이 없다고 판단되는 문헌 1,700편과 국문 또는 영어가 아닌 제2외국어로 작성된 문헌 9편을 제외하였다. 2차 문헌 선택/배제 과정에서는 103편의 문헌에 대한 전문 검토를 통해 응급구조사 보수교육과 직접적으로 관련성이 없다고 판단되는 문헌 46편과 원저가 아닌 문헌 26편, 전문을 구할 수 없는 문헌 6편을 제외하였다. 2차 문헌 선택/배제를 통해 선정된 문헌은 25편이었고, 25편의 문헌에서 인용한 참고문헌을 토대로 수기검색을 시행하였다. 기존 키워드를 통해 검색되지 않는 문헌 1편을 수기 문헌으로 추가하여 총 26편의 문헌이 최종 분석에 포함되었다<Fig. 1>. 응급구조사 보수교육 관련된 문헌 26편 중 국내 문헌은 9편, 국외 문헌은 17편이었다.

3. 논문의 비뚤림 위험 평가
최종 선정된 26편의 문헌을 대상으로 비뚤림 위험 평가를 수행하였다. 비뚤림이란 체계적인 오류로 인해 결과가 참값으로부터 벗어나 있는 것을 의미하며, 연구 설계에 따라 비뚤림 위험 평가 도구를 선정하여 최종 선정된 개별 문헌의 비뚤림 위험을 평가할 수 있다[11]. 본 연구에서 선정된 문헌은 질적 연구와 양적 연구가 모두 포함되어 있기 때문에 이를 평가하기 위하여 정량적, 정성적 연구를 모두 평가할 수 있도록 개발된 Qualsyst 도구를 활용하였다[12]. Qualsyst 도구는 캐나다 의료연구재단 AHFMR (Alberta heritage foundation for medical research)에서 개발한 실용적이고 체계적 검토 도구로 유용성과 타당성이 입증되었고, 다양한 연구 설계 방법에서 유용하게 사용할 수 있다는 장점이 있다[13]. 본 도구를 활용하여 26편의 문헌을 정량적 평가 기준과 정성적 평가 기준으로 나눴을 때 정량적 평가 기준에 해당하는 문헌은 22편, 정성적 평가 기준에 해당하는 문헌은 5편이었다. 이 중 정량적, 정성적 연구를 모두 수행한 연구는 1편이었으며, 이 연구에는 정량적 평가와 정성적 평가를 모두 시행하였다. Qualsyst 도구 평가 기준은 정량적 연구의 경우 총 14개의 평가 기준이 있으며 기준에 적합한 경우 2점(Yes), 부분적으로 적합한 경우 1점(Partial), 기준에 적합하지 않은 경우 0점(No)을 부여하였고, 해당 없는 경우 Not applicable(N/A)로 분류하였다. 정성적 연구는 총 10개의 평가 기준이 있으며 기준에 적합한 경우 2점(Yes), 부분적으로 적합한 경우 1점(Partial), 기준에 적합하지 않은 경우 0점(No)을 부여하였다. 이 과정은 두 명의 연구자가 독립적으로 수행하였으며 두 연구자 간의 의견 불일치가 발생하는 경우 공동연구자(제3자)와의 논의를 거쳐 최종적으로 평가 결과를 도출하였다.
정량적 연구에서는 입력변수에 대한 자료 선택 도구 설명 평가에서 1편의 연구가 적절하지 않은 선택 도구를 선정하였고, 변수 추정 값의 경우 2편에서 결과표와 결과 기술에서 상이한 결과를 제시하였다. 혼란 변수 중재의 경우 1편에서 공분산 분석을 시행하였으나 보정 변수에 대해 언급하지 않았다. 연구 결과에서는 2편이 결과 기술 오입력으로 부적절한 해석을 제시하였으며, 결론의 경우 3편의 연구에서 결과를 통해 설명되지 않는 부분을 언급하였다<Table 1>.
Table 1
Quality assessment quantitative studies
정성적 연구에서는 1편의 논문에서 연구의 목적, 연구 설계, 정보 수집 전략, 정보 수집 방법, 분석, 신뢰성 검증 절차, 결론 제시를 명확하게 언급하지 않았으며, 이 외에도 데이터 수집과 분석에 대해 언급하지 않은 논문 1편, 신뢰성 검증 절차에 대해 언급하지 않은 논문 1편이 있었다<Table 2>.
Table 2
Quality assessment qualitative studies
Ⅲ. 연구결과
1. 연구 유형에 따른 응급구조사 보수교육 연구 동향
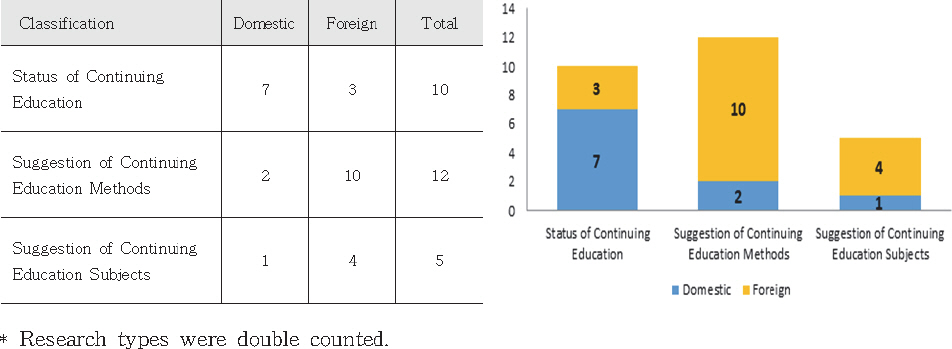
응급구조사 보수교육 연구 유형은 보수교육 실태 조사, 보수교육 방법 제시, 보수교육의 과목 제안의 비교로 대별할 수 있었다.
보수교육 실태 조사를 시행한 총 10편의 문헌 중 7편은 국내 문헌, 3편은 국외 문헌이었다. 10편의 문헌 중 9편은 설문조사를 실시하였고, Shin 등[6]의 연구만이 비교분석(comparative analysis)을 시행하였다. 보수교육의 방법을 제시한 문헌은 총 12편으로 국내 문헌 2편, 국외 문헌이 10편이었다. Choi 등[8]의 연구는 보수교육 방법 제안을 연구 목적으로 설정하였으나, 문헌 내에서 보수교육 실태 조사와 보수교육 방법 제시 두 가지를 모두 수행하였기에 연구 유형에서는 중복으로 산정하였다.
보수교육 과목에 대해 제안한 문헌은 총 5편으로 국내 문헌 1편, 국외 문헌이 4편이었다<Fig. 2>.
2. 발행 시기별 응급구조사 보수교육 연구 동향
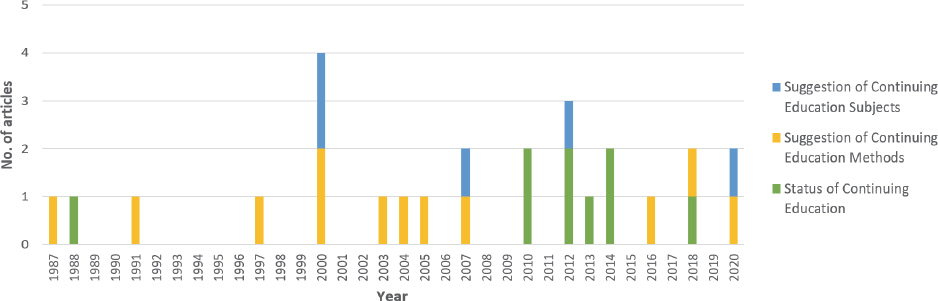
국내·외 응급구조사 보수교육과 관련된 학술 문헌은 1987년부터 2020년까지 총 26편이 발행되어 전반적으로는 적은 추세였으나, 최근까지도 연구가 진행되었음을 알 수 있다. 특히, 2000년의 경우 4편이나 발행되어 다른 시기보다 발행 비중이 높았다. 응급구조사 보수교육 방법을 제안한 학술 문헌은 1987년 초기부터 현재까지 지속적으로 연구되고 있음을 알 수 있으며, 2010년부터 2014년 사이에는 응급구조사 보수교육 실태 조사에 관한 연구가 활발히 진행된 것을 확인할 수 있다. 한편, 보수교육 과목을 제안하는 연구는 2000년부터 시작되어 현재까지 산발적으로 발행되고 있다<Fig. 3>.
3. 응급구조사 보수교육의 유형별 분석 결과
1) 보수교육 실태 조사
보수교육 실태를 파악하기 위해 자료를 수집한 지역적 범위는 국내의 경우 경기도가 4회, 서울특별시, 경상남도 마산시, 강원도가 2회 조사 되었으며, 그 외에 대구광역시, 대전광역시, 광주광역시, 부산광역시, 인천광역시, 제주특별자치도, 경상북도, 충청도가 1회씩 조사 지역으로 선정되었다. 국외의 경우 미국 캘리포니아에서 실시된 연구에서는 주 라이센스 리스트와 메일 리스트를 활용하여 Paramedic에게 설문조사를 요청하였고[15], 아일랜드는 아일랜드에 등록된 모든 EMT와 Paramedic에게 설문조사를 요청하였다[16, 17]<Table 3>.
Table 3
Data source and analysis unit / number of observations
| Author (Year) | Data collection country (Area) | Analysis method | Year of data collection | Number of survey subjects | Number of response surveys | Domestic | Foreign | ||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| 1'st emergency | 2'nd emergency medical technician medical technician | EMT | Paramedic | ||||||
| Roberts et al. (1988) [15] | United states of america (California) | Survey analysis | - | 352 | 17 | - | - | - | 17 |
|
|
|||||||||
| Choi ct al. (2003) [8] | Republic of korea (Gyeonggi/ Gangwon/ Incheon) | Survey analysis | 2002 | 290 | 290 | 90 | 200 | ||
|
|
|||||||||
| Kim et al. (2010) [9] | Republic of korea (Seoul/ Gyeonggi) | Survey analysis | 2010 | 476 | 476 | ||||
|
|
|||||||||
| Shin et al. (2010) [6] | - | Comparative analysis | - | - | - | - | - | - | - |
|
|
|||||||||
| Bae et al. (2012) [7] | Republic of korea (Seoul/Gyeonggi/ Daejeon/Gwangju/ Busan/Masan/Jeju) | Survey analysis | 2010 | 389 | 389 | 295 | 94 | - | - |
|
|
|||||||||
| Rho et al. (2012) [18] | Republic of korea (Daegu/ Gyeongbuk) | Survey analysis | 2010 | 299 | 215 | 114 | 101 | - | - |
|
|
|||||||||
| Knox et al. (2013) [16] | Ireland | Survey analysis | 2012 | 399 | 399 | - | - | 399 | - |
|
|
|||||||||
| Knox et al. (2014) [17] | Ireland | Survey analysis | 2012 | 789 | 789 | - | - | - | 789 |
|
|
|||||||||
| Hong et al. (2014) [2] | Republic of korea (Masan) | Survey analysis | 2014 | 150 | 150 | 108 | 42 | - | - |
|
|
|||||||||
| Park et al. (2018) [4] | Republic of korea (Gyeonggi/ Chungcheong /Gangwon) | Survey analysis | 2018 | 222 | 222 | 146 | 76 | - | - |
보수교육 만족도의 경우 ‘업무 능력 향상에 도움이 되었는가?’를 묻는 연구는 국내의 3개 문헌이 있었으며 세 개의 문헌에서 공통적으로 만족도가 낮았다[2, 8, 9]. 또한, 직군별로 비교했을 때, 2급 응급구조사보다 1급 응급구조사의 보수교육 만족도가 낮게 나타났으며[4, 7] 특히 의료기관에 근무하는 1급 응급구조사의 경우 보수교육 시간에 대한 만족도, 방법에 대한 만족도, 주제에 대한 만족도 모두 소방에서 근무하는 응급구조사보다 낮았다. 한편, 연령대가 낮고, 근무 기간이 적은 경우에도 만족도가 낮았다[7].
보수교육 시간의 경우 국외에 비해 국내의 보수교육 시간이 월등히 낮은 것을 확인할 수 있었다. 국내의 경우 대부분 연 1회, 주 4시간 정도를 참여하는 것으로 확인되었지만 국외의 경우, 미국은 DOT 국가 표준 기준 72시간, 일본은 2년간 128시간을 권고하고 있으며[6] 아일랜드 EMS 종사자의 대부분은 연 20시간 이하의 보수교육을 참여하고 있었다[16, 17].
희망 보수교육 시간의 경우 국내에서는 4시간 미만을 제시한 경우가 3편[2, 8, 9], 4-8시간 미만을 제시한 경우가 1편 있었고[7], 국외에서는 아일랜드의 경우 희망 보수교육 시간이 21-40시간이었다[16, 17].
가장 희망하는 프로그램은 국내의 경우 기본인명 소생술, 전문 인명 구조술, 제세동기, 호흡기계 응급처치, 특수상황 응급처치, ALS, 출혈과 쇼크, 다발성 외상환자 처치였으며, 문헌별로 상이하였다. 국외의 경우 미국 캘리포니아에서는 비 임상적인 과목으로 업무 스트레스와 번아웃 증후군, 임상적인 과목으로서는 심혈관 질환, 유해물질 취급 및 약물 투여 방식에 대한 교육 프로그램을 희망하였다. 아일랜드는 실제 시나리오를 접목한 교육을 희망하였다.
희망 학습 방법으로는 국내의 경우 강의와 실습의 병행을 원하는 문헌이 3편이었다[4, 9, 18]. 이 중 1편은 병원 구조사의 경우가 강의와 실습의 병행을 원하였고, 소방 구조사의 경우 온라인 교육을 선호하였다[4]. 강의식 교육을 온라인 교육보다 선호한다는 문헌은 1편이 있었다[2]. 학습 프로그램에 관하여 보수교육 내용의 질적 개선을 요구하는 문헌이 1편[7], 현장실무 위주의 교과 내용 개편을 요구하는 문헌이 1편[8], 1급과 2급 응급구조사의 보수교육 분리를 요구하는 문헌이 1편 있었다[4]. 국외의 경우 e-러닝을 포함하는 혼합 학습 전략과 강제적 요소와 자발적 요소를 모두 지닌 프로그램에 대해 요구하는 문헌이 각각 1편씩 있었다[16, 17]<Table 4>.
Table 4
Status of continuing education
| Author (Year) | Evaluation of continuing education | ||||
|---|---|---|---|---|---|
|
|
|||||
| Satisfaction with continuing education | Training hours/count | Number / time of desired remuneration training | The most wanted subject of continuing education. | Desired learning method | |
| Roberts et al. (1988) [15] | - | - |
- Non clinical issues : job-stress/burn-out - clinical issues : Cardiovascular disease, handling and administration of hazardous substances |
- | |
|
|
|||||
| Choi et al. (2003) [8] | - The degree to which it is helpful in practice ’Complaints (very unsatisfactory + unsatisfactory) 30.4%’, ’Normal 38.3%’ | - | Once a year, 4 hours (48.0%) |
- Basic life support (93.7%) - Clinical emergency : Bleeding and shock (92.1%) |
Field-oriented curriculum contents (43.0%) |
|
|
|||||
| Kim et al. (2010) [9] |
- 119 Paramedic’s Continuing education does not reflect the needs of paramedics. - 55.1% Of ’respondents did not know’ and ’did not help improve their work’. |
- Participation at least once a year, not more than three times a year (54.0%) - More than 4 hours-less than 5 houre (45.1%) |
- Conducted once a year (41.6%) - Less than 4 hours (67.2%) |
BLS(Basic life support) | Lecture + Practice |
|
|
|||||
| Shin et al. (2010) [6] | - |
- Korean completion standard : more than 4 hours a year - American completion standards : it varies from state to state / 72 hours total based on DOT national standard - Japan completion standards : 1 hour for 2 years is converted to 1 hour, at least 128 hours (recommended) |
- | - | - |
|
|
|||||
| Bae et al. (2012) [7] | - 1st emergency medical technical are less satisfied with maintenance training than 2’nd emergency medical technical personnel. | Participate each year (62.0%) | More than 4 hours - less than 8 hours (63.2%) | ALS(Advanced Life Support) (40.0%) | - Quality improvement of education |
|
|
|||||
| Rho et al. (2012) [18] | - Participation once a year (44.1%) | Conducted once or twice a year (31.1%) - 4 times a year (31.1%) | Automatic external defib-rillator method (73.9%) | Theory + Skill | |
|
|
|||||
| Knox et al. (2013) [16] | - | - 20 hours or less per year (24.0%) | 21-40 hours a year (25.0%) | - Practical training scenarios (97.0%) | Paramedics and advanced paramedics and a blended learning approach with e-learning. |
|
|
|||||
| Knox et al. (2014) [17] | - | - 20 hours or less per year (27.6%) | 21-40 hours a year (35.0%) | - Practical training scenarios (94.0%) | Mixed model approach of CPC (compulsory+spontaneously) |
|
|
|||||
| Hong et al. (2014) [2] | - Capability improvements help (’normal’ and ’no’ percent 52.0%) | - | Blow 4hour (65.3%) |
- Respiratory system emer-gency measures (12.0%) - Special emergency meas-ures (12.0%) |
- Lecture training 50.0% - Off-line training 42.7% |
|
|
|||||
| Park et al. (2018) [4] |
- Continuing education according: Time satisfaction : * Hospital EMT-I < 119 EMT-II - Continuing education according : Method satisfaction: * 119 EMT-I ,II> Hospital EMT. * Career ≥8 < ≤ 13 - Continuing education according- Topic satisfaction: * Hosipital EMT-1 < medical EMT I ,II * Career ≥8 < ≤ 13, * Age 20s < 40s |
- | - | - Assessment and management of multiple trauma patient |
- Continuing education Job characteristics: Separation 119 EMT-1, 119 EMT-n - Needs of continuing education topics: * Hospital EMT: Theory+practical training * 119 EMT: Off-line training |
2) 보수교육 방법 제안
보수교육 방법을 제안한 문헌은 국내 문헌이 2편, 국외 문헌이 10편이었다. 국외 문헌 중 자료수집 국가를 명확히 알 수 있었던 문헌은 9편이었으며 미국이 7편, 캐나다가 1편, 인도는 1편이었다. 보수교육 학습 도구에 대해 언급한 문헌은 총 5편이었으며, 교육 프로그램에 대한 개선을 언급한 문헌은 8편이었다. Lindquist 등[14]의 연구는 학습 방법과 교육 프로그램을 모두 제시하였다. 연구자들이 제안하는 보수교육 방법은 환자 사례 발표를 통한 피드백 교육이 4편[14, 19-21]으로 가장 많았다. 온라인을 활용한 교육의 효과성 및 제안은 3편[22-24], 보수교육 개발에 있어 참여자를 고려하고, 보수교육에 대한 평가를 시행하자는 제안은 3편이었다[8, 14, 25]. 또한 소셜미디어 플랫폼의 활용[26], 응급구조사는 의사 결정시 이성적 사고를 선호한다라는 사실을 보수교육 프로그램 개발 시 반영하는 것에 대한 제안[27], 응급구조사는 초기교육, 보수교육, 병원 전 처치에서 모두 술기에 대해 대부분 중요하다고 느끼기 때문에 프로그램 개발 시 고려해야 한다[28]는 제안이 각각 1편씩 있었다<Table 5>.
Table 5
Suggestion of continuing education methods - to be continued
| Author (Year) | Data collection country (Subject) | Analysis method | Year of data collection | Number of survey subjects | Number of response surveys | Training Proposal | The author’s proposed method of conservative education |
|---|---|---|---|---|---|---|---|
| Zautcke et al. (1987) [25] | United States of America (Chicago: paramedic) | Evaluate education and training | - | 40 | 40 | Program tools | - The continuing education and recertification process need to develop reliable methods to identify and then correct deficiencies in performance levels of system participants. |
|
|
|||||||
| Porter. (1991) [22] | United States of America (Michigan: paramedic) | Survey analysis | - | 111 | 111 | Learning tools | - Computer-aided education has been shown to be effective during the period of acquiring and retaining knowledge about the remuneration education of emergency responders. |
|
|
|||||||
| Pollock et al. (1997) [28] | United States of America (North Carolina : 41 EMS agencies paramedic) | Survey analysis | - | 600 | 600 | Program tools |
- The three skills that the first aid worker evaluated as the most important in early education, maintenance education, and pre-hospital treatment were intubation, defibrillation, and patient evaluation in the institution. - Should be considered in developing patient care protocols and EMS education programs, as well as in the revision process for the paramedic National Standard Curriculum.. |
|
|
|||||||
| Ryu et al. (2000) [21] | Republic of Korea (Records of patients visiting the emergency room of hospital b through the fire service in northeastern seoul) | Collect first-aid journal | 1999 | 1,882 | - | Program tools |
- When quality control was implemented before the hospital, the suitability of first aid workers was increased and the nonconformity was reduced. - Feedback training on first aid should be provided. |
|
|
|||||||
| Wilson. (2000) [19] | - | - | - | - | - | Program tools |
- Encourage active participation through patient case presentation. - Establish open forum time for post-training questions and discussions. |
| Choi et al. (2003) [8] | Republic of Korean (Gyeonggi/ Gangwon/Inchean: paramedics) | Comparative analysis & Survey analysis | 2002 | 290 | 290 | Program tools |
- The number of courses should be increased and the content should be subdivided. - Reasonable class hours for each subject should be allocated. - A curriculum applicable to field work should be organized. - Education opportunities should be expanded by increasing the number of refresher training sessions. - The educational conditions should be improved, and educational outcomes should be evaluated and returned. - Based on the assessment data, it should be reflected in the following curriculum |
|
|
|||||||
| Miler et al. (2004) [20] | United states of America (National council of state emergency medical, Emergency nurses association, National association of EMS physicians, National association of EMTs, The national registry of EMTs, National association of EMS educators, The national highway traffic safety administration- EMS division, and the maternal and Child health bureau) | Expert opinion + Literature Review | - | - | - | Program tools |
- A pediatric competency-based continuing education program is implemented to sustain proficiency in knowledge and skills for out-of-hospital providers. - Providers should receive frequent and accurate feedback on performance during pediatric skills practice to establish psychomotor skills competency. - Pediatric continuing education methodology is based on individual learning styles. - Continuing education can be classified dynamically and statically, dynamic classification is a methodology in which interaction is made and static classification is a methodology that lacks interaction opportunities, both of these categories have proven valuable in establishing learner competencies and should be considered when creating continuing programs. |
|
|
|||||||
| Jerin et al. (2005) [24] | United states of America (King county, Washington: EMT) | Survey analysis | 2002 | 391 | 391 | Learning tools |
- Three-quarters of emergency respondents who responded to the survey preferred Web-based education (WBT) over traditional teaching methods. - The advantages to the user and the fire agency over traditional training include EMT convenience, ease of scheduling training, flexibility in learner requirements consistent delivery of content, multiple opportunities for review, ease of evaluation and easier record keeping and administration. |
|
|
|||||||
| Lellis et al. (2007) [23] | United states of america (North Carolina: 8 County-based emergency management system) | Survey analysis | 2003 | 358 | 208 (EMS) | Learning tools |
- Online education about Stroke worked. - We suggest that online education is a wise investment. |
| Jensen et al. (2016) [27] | Canada (Nova scotia, New brunswick, Ontario: paramedic) | Survey analysis | 2012 | 1,172 | 904 | Program tools | - Care paramedic students at entry to practice level, we found paramedics and paramedic students prefer and perceive that they have the ability to use rational over experiential thinking. This information adds to our current knowledge on paramedic decision-making and is potentially important for developing continuing education and clinical support tools. |
|
|
|||||||
| Mason et al. (2018) [26] | - | Contents analysis | 2014-2017 | - | - | Learning tools | - Use among paramedics and other prehospital care clinicians is on the rise and is increasingly being used as a platform for continuing education and international collaboration. It is used for the sharing of emergency medical services, paramedicine, and prehospital care- related content. |
|
|
|||||||
| Lindquist et al. (2020) [14] | India (Telangana, Gujarat, Karnataka, Himachal Pradesh: EMT) | Survey analysis | 2014-2017 | 504 | 504 | Learning tools & Program tools |
- Use minimal text and animation when using presentation media. - Combining workbooks during lectures and video lectures improves participation. - Programs focusing on active learning exercises, including simulation and case discussion, should be built. - Observation, evaluation, feedback, and course of instructor training It is important. - On several occasions, EMT instructors or course participants suggested changes to educational content during piloting of each program, (such flexibility allowed all partners to tailor the course to the exact needs of the learners, and in particular, the clinical context in which they work) |
3) 보수교육 과목 제안
보수교육 과목을 제안한 문헌은 총 5편이었으며 이 중 국내 문헌이 1편이었고, 국외 문헌은 4편이었으며 4편 모두 미국에서 설문조사를 실시한 문헌이었다. 국내의 경우 법의학 교육을 제안하였다[29]. 법의학 교육에 대한 설문조사 결과로 ‘보수교육에서 실시했으면 좋겠다’는 응답이 가장 높게 나타난 것을 확인할 수 있었다. 국외의 경우 노인에 대한 교육[30], 소아 응급처치[31], 특수 관리가 필요한 아동에 대한 교육[32], 사망 통보와 관련된 표준화된 훈련[33]이 보수교육 과목으로 필요하다고 제안하였다<Table 6>.
Table 6
Suggestion of continuing education subjects
| Author (Year) | Data collection country (Subject) | Analysis method | Year of data collection | Number of survey subjects | Suggested subject for mntinuing education |
|---|---|---|---|---|---|
| Glaeser et al. (2000) [31] | United states of America (EMS provider registered with NREMT) | Survey analysis | 1997 | 18,218 | - Pediatric first aid education |
|
|
|||||
| Spaite et al. (2000) [32] | United states of America (National registered of EMTs paramedics employed by a municipal fire department) | Survey analysis | - | (Pre-training) 41 (Post-training) 49 | - Pediatric advanced life support (PALS) or other specialized pediatric training. |
|
|
|||||
| Kim et al. (2007) [29] | Republic of Korea (Seoul, Busan, Daegu, Ulsan, Gyeonggi-do, Gyeongsang-do: EMT) | Survey analysis | 2007 | 307 | - Forensic education |
|
|
|||||
| Shah et al. (2012) [30] | United states of America (a two-county region around Rochester, New York, that includes urban, suburban, and rural areas were targeted: EMS providers) | Survey analysis | 2008-2009 | 6,066 | - Geriatric education program |
|
|
|||||
| Campos et al. (2020) [33] | United states of America (EMS Professional registered with NREMT) | Survey analysis | 2017 | 1,514 | - Standardized training related to death notification |
Ⅳ. 고찰 및 결론
1. 주요 결과 및 고찰
본 연구는 응급구조사 보수교육에 관한 연구들을 체계적으로 고찰하여 응급구조사 보수교육의 실태와 보수교육에 대한 제안을 종합하고자 하였다. 체계적 문헌고찰의 주요 결과는 다음과 같다.
첫째, 응급구조사 보수교육에 대한 만족도가 낮았다. 만족도가 낮은 이유로는 보수교육 프로그램에 참석자의 요구가 반영되지 않는다는 점과 실무와 연관 없는 교과편성이 이루어지고 있으며 내용의 질적 개선이 필요하다고 느끼기 때문인 것으로 나타났다. 이에 관하여 보수교육 제안에 관한 문헌에서도 보수교육 프로그램 개발에 있어 참석자의 요구 및 실태를 파악하여 개발해 나갈 것을 제안하고 있다. 희망 학습 방법은 강의와 실습의 병행이 가장 많이 제안되었으나 현재까지도 전통적인 강의식으로 교육이 이루어지고 있어 이 또한 참여자의 요구가 반영되지 않고 있다는 것을 확인할 수 있었다. 한편, 현재 보수교육 참여 시간과 희망 보수교육 시간 모두 국외에 비해 낮았는데, Choi 등[8]의 연구에 따르면 교육을 참석하기 위해서 비번에 참석하거나 업무 일정 조정의 필요성 등으로 인해 참석의 어려움을 느끼는 경우가 있는 것으로 보인다. 이는 온라인 교육의 활성화와 Lindquist 등[14]의 연구에서 제안하는 바와 같이 워크북 형태를 결합하여 참여도를 향상시키는 방법 또는 다양한 플랫폼을 활용하여 개선할 수 있을 것이다.
둘째, 보수교육 방법에 대해 가장 많이 제안된 방법은 환자 사례 발표였다. 이를 통해 적극적인 참여를 유도하고 피드백을 통해 응급처치의 적합도를 높일 수 있다고 밝혔으나 현재까지는 반영되지 않고 있어 이에 대한 검토가 필요할 것이다. 또한, 보수교육 자체에 대한 평가를 시행하자는 문헌들을 토대로 강사에 대한 관찰, 평가, 피드백 등을 시행하고 평가 자료를 기반으로 차기 교육 과정에 반영하여 지속해서 보수교육을 개선해 나가야 할 것이다.
셋째, 보수교육에서 제안하고 있는 교육 과목들과 대상자들이 희망하는 보수교육 프로그램은 공통점 없이 다양하였다. 이는 대상자의 특성에 따라 요구하는 교육 프로그램의 차이가 있을 수 있다는 것을 설명한다. 특히 의료기관에 있는 1급 응급구조사의 보수교육 만족도는 소방에 있는 응급구조사보다 낮게 나타났다. 연령은 낮고 근무 기간이 적을수록 만족도가 낮게 나타나는 것을 확인할 수 있었다. Park과 Yoon[4]의 연구에서도 1급과 2급 응급구조사의 보수교육 분리가 필요하며 보수교육 주제와 방법의 다양화를 통해 원하는 주제를 선택할 수 있도록 해야 한다고 언급하였다. 이처럼 대상자들의 특성에 따라 요구도의 차이가 발생하고 있는데, 이와 관련하여 Shin 등[6]의 연구에서는 평점 인정제도를 도입하는 것을 제안하였고, Knox 등[17]의 연구에서도 기본적인 교육에 참석하는 강제적 요소와 자신에게 적합한 프로그램에 참여하는 자발적 요소를 더한 보수교육을 희망한다고 밝히고 있어 이에 대한 고려가 이루어져야 할 것이다.
마지막으로는 보수교육에 대한 연구가 지속해서 이루어지지 못하고 있는 것으로 나타났다. Park과 Yoon[4]에 따르면 보수교육의 질 관리를 위해서는 교육 요구에 대해 파악하고 반영해야 한다고 하였으나 만족도 조사에 관한 국내 연구는 총 6편으로 가장 최근의 국내 연구는 2018년의 연구여서 지속적인 만족도 조사는 이루어지지 않고 있음을 알 수 있다. 또한, 응급구조사 보수교육에 대한 만족도는 여전히 낮은 것을 확인하였다. 이에 보수교육에 따른 만족도와 업무능력 향상에 대해 지속적인 연구가 필요할 것이다.
2. 연구의 한계 및 의의
국외와 달리 국내 보수교육 연구는 설문조사를 실시한 모든 문헌에서 공통적으로 전국적인 조사가 실시되지 않아 일반화의 어려움이 있다고 언급하였다[2, 4, 7-9, 18, 29]. 이에 본 연구에서 제시한 결과 또한 일반화를 할 수 없다는 제한점이 있었다. 그뿐만 아니라 만족도 및 역량 강화 여부에 대한 조사가 국내에서는 지속적으로 이루어지고 있지 않아 최신 현황을 반영하기에는 어려움이 있다. 그러나 체계적 문헌 고찰을 통해서 단일 문헌에서 제시한 결과보다는 종합적인 결과를 도출할 수 있었고 본 연구를 통하여 전국적인 보수교육의 만족도 조사와 역량 강화 여부에 대한 지속적인 조사 및 연구의 필요성에 대해 시사했다는 점에서 그 의의가 있다.
3. 결론
응급환자에게 최선의 처치를 제공하기 위해 응급구조사의 적절한 보수교육은 필수적이었으나 응급구조사 보수교육에 관한 체계적 문헌 고찰을 실시한 결과 업무 능력 향상과 만족도는 낮게 나타난 것을 확인할 수 있었다. 이를 개선하기 위해서는 교육 대상자들의 요구를 지속적으로 수집하고 반영하며, 보수교육을 평가하여 프로그램을 개선해나가는 노력이 필요하다. 또한 응급구조사 특성에 따른 다양한 프로그램을 제공하고, 보수교육 점수를 인정하는 방안에 대해서도 고려가 필요하다. 보수교육 참석이 어려운 경우에는 다양한 플랫폼 및 온라인 학습 방법을 개발하여 참여도와 만족도는 높이고 보수교육에 대한 참석 방안을 늘리는 방법에 대해서도 지속적으로 개발해나가야 한다. 마지막으로 앞으로 보수교육에 대한 전국적인 조사와 지속적인 연구가 적극적으로 이루어져야 한다는 것을 제안하는 바이다.




