3인 CPR 프로토콜 개발 및 타당도 검증
Development and validation of a three-person cardiopulmonary resuscitation protocol
Article information

Trans Abstract
Purpose:
This protocol aims to improve the simplicity of the existing two-person cardiopulmonary resuscitation (CPR) by focusing on chest compressions and artificial respiration, and classifying the roles within the scope that can be observed.
Methods:
In this study, the protocol was developed by forming an expert group consisting of a professor from the emergency and rescue department, a professor from the nursing department, and a first aid officer from the fire department. In addition, if the number of panels is 15 and the derived content validity ratio (CVR) value exceeds 0.49, a reference point that satisfies content validity at 95% reliability is presented.
Results:
All 11 performance items exceeded the CVR value of 0.49 to meet the reference point, and the CVR range of this protocol is 0.625 to 1.000.
Conclusion:
In order to improve the quality of three-person CPR, verification of simulation models and continuous protocol revision should be conducted by individuals specializing in various fields.
Ⅰ. 서 론
최근 개최한 급성심장정지조사 심포지엄의 발표 자료에 의하면 2020년 119 구급대가 이송한 급성심장정지 환자는 총 3만 1,652명이었고, 그 중 7.5%인 2,345명이 생존하였다. 이는 전년 대비 약 1.2% 감소한 수치이며, 환자의 뇌기능 회복률 역시 2019년의 5.4%에서 4.9%로 감소하였다. 또한 일반인 심폐소생술(cardiopulmonary resuscitation, CPR)이 제공된 환자는 26.4%로 과거와 비교하였을 때 지속적으로 증가하는 추세이지만, 목격된 급성심장정지가 50.1%라는 조사 결과에 비추어 보면 일반인의 경우 심장정지를 목격하였음에도 심폐소생술을 시행하지 않은 경우가 대다수였음을 알 수 있다[1].
심장정지 환자의 생존율에는 적절한 가슴압박과 인공호흡이 얼마나 빠르게 시행되었는지가 무엇보다 중요하며, 특히 병원 전 환경에서는 목격자에 의한 빠른 심폐소생술 실시 및 구조자의 수 등이 심폐소생술의 질에 영향을 미치게 된다[2]. 실제로 우리나라는 목격자에 의한 심폐소생술 시행률을 증가시키기 위해서 전 국민을 대상으로 심폐소생술 교육을 확대하고 홍보를 강화하는 등의 정책을 도입하였고, 소방청은 구급대원의 인력증가가 심장정지 환자의 생존율 증가에 중요하다고 판단하여 2014년부터 ‘119구급차 3인 탑승제도’를 실시하였다[3]. 이처럼 소방공무원은 심장정지 환자의 생명을 결정짓는데 중요한 역할을 담당하고 있음을 고려한다면, 이들을 대상으로 보다 명확하고 세분화된 업무 분담을 제시할 수 있는 교육 프로토콜이 필요하며 그에 따른 평가용 체크리스트가 만들어져야 한다.
현재 심폐소생술 교육과 관련하여 미국심장협회(American Heart Association, AHA)와 대한심폐소생협회에서 주최하는 기본소생술 과정과 한국기본소생술 과정, 일반인 심폐소생술 과정에서의 프로토콜 및 평가용 체크리스트가 공식적으로 사용되고 있다[4, 5]. 그러나 이는 1인 및 2인 구조자의 경우로 한정되어 있고 구조자의 수에 대한 세부적인 업무분담 내용이 포함되어 있지 않다. 실제 상황에서는 2인 이상이 소생술에 참여하는 경우가 대부분이고 특히 3인 출동 체제가 이루어지고 있다는 것을 감안할 때, 3인 구조자 환경에서의 팀워크 유지, 의사소통 등에 대한 교육 내용을 담고 있는 3인 심폐소생술 프로토콜 개발이 필요하다.
3인 심폐소생술 프로토콜은 심폐소생술 경험이 많은 소방공무원에게는 팀 내에서의 업무 중복을 피할 수 있도록 명확한 역할분담을 제시하고, 비교적 경험이 적은 신임 소방공무원이나 구급대원이 아닌 타 직렬의 소방공무원에게는 교육적인 도구로 사용함으로써 소생술 동안 수행해야 하는 세부적인 역할의 이해도를 높일 수 있다. 결과적으로 심폐소생술 전체 과정에 대한 정확한 이해와 함께 소생술 업무의 체계성을 확보할 수 있으므로 심장정지 환자에게 양질의 심폐소생술을 제공할 수 있을 것이다.
따라서 본 연구는 병원 전 심장정지 상황에서 펌뷸런스 대원을 포함하는 소방공무원 역할이 구체적이고 명확하게 구분된 3인 심폐소생술을 시행하는데 필요한 프로토콜을 개발하고자 한다. 더 나아가 본 프로토콜의 사용으로 소방공무원의 합동훈련, 신임 소방학교 교육훈련 등 소방공무원을 위한 심화된 심폐소생술 교육자료를 개발하는데 기초자료를 제공하고자 한다.
Ⅱ. 연구방법
1. 연구설계
본 연구는 3인 CPR 프로토콜을 개발하기 위해 수행 항목을 작성하고, 3인 CPR 프로토콜에 대한 전문가 집단의 타당도를 검증하여 개발된 프로토콜의 적정성을 평가하는 방법론적 연구이다.
2. 프로토콜 개발 목표
본 프로토콜은 기존 가슴 압박과 인공호흡에 중점을 둔 2인 CPR의 단순함을 개선하고, 심정지 환자의 현장에 1인, 2인, 3인의 목격 가능한 범위 내에서의 역할을 구분하여 프로토콜화 하고자 한다. 또한, 신임 소방공무원 구급 실무 교육 시 기본과정으로 편성하여 구급대원이 아니더라도 교육, 훈련의 대상을 현장에서 생활 안전 업무를 담당하고 있는 펌뷸런스 대원 등으로 확대하여 좀 더 체계적이고 심화된 심폐소생술 교육자료를 개발하는데 기여하고자 한다<Table 1, Table 2>.
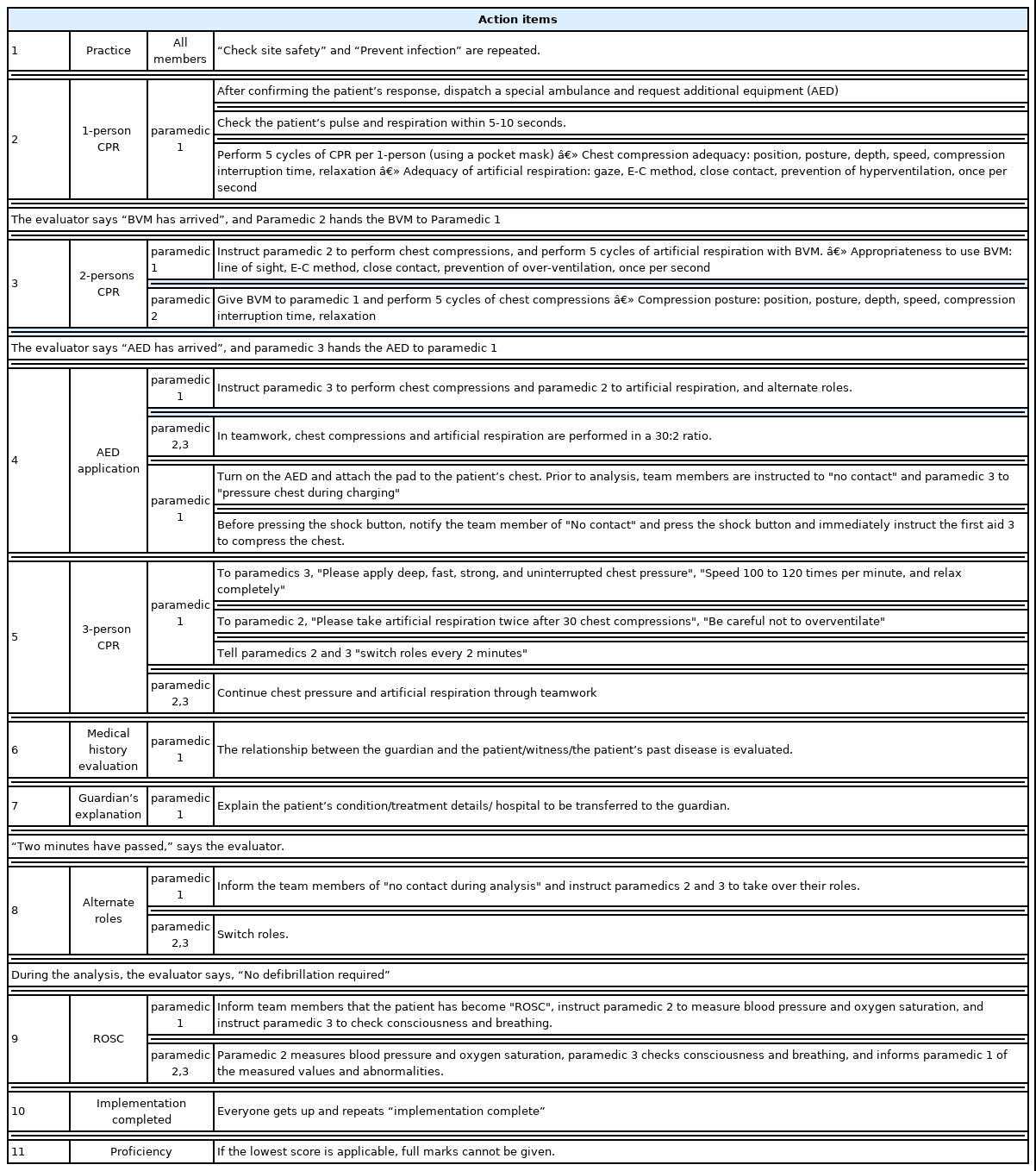
Three-persons CPR protocol
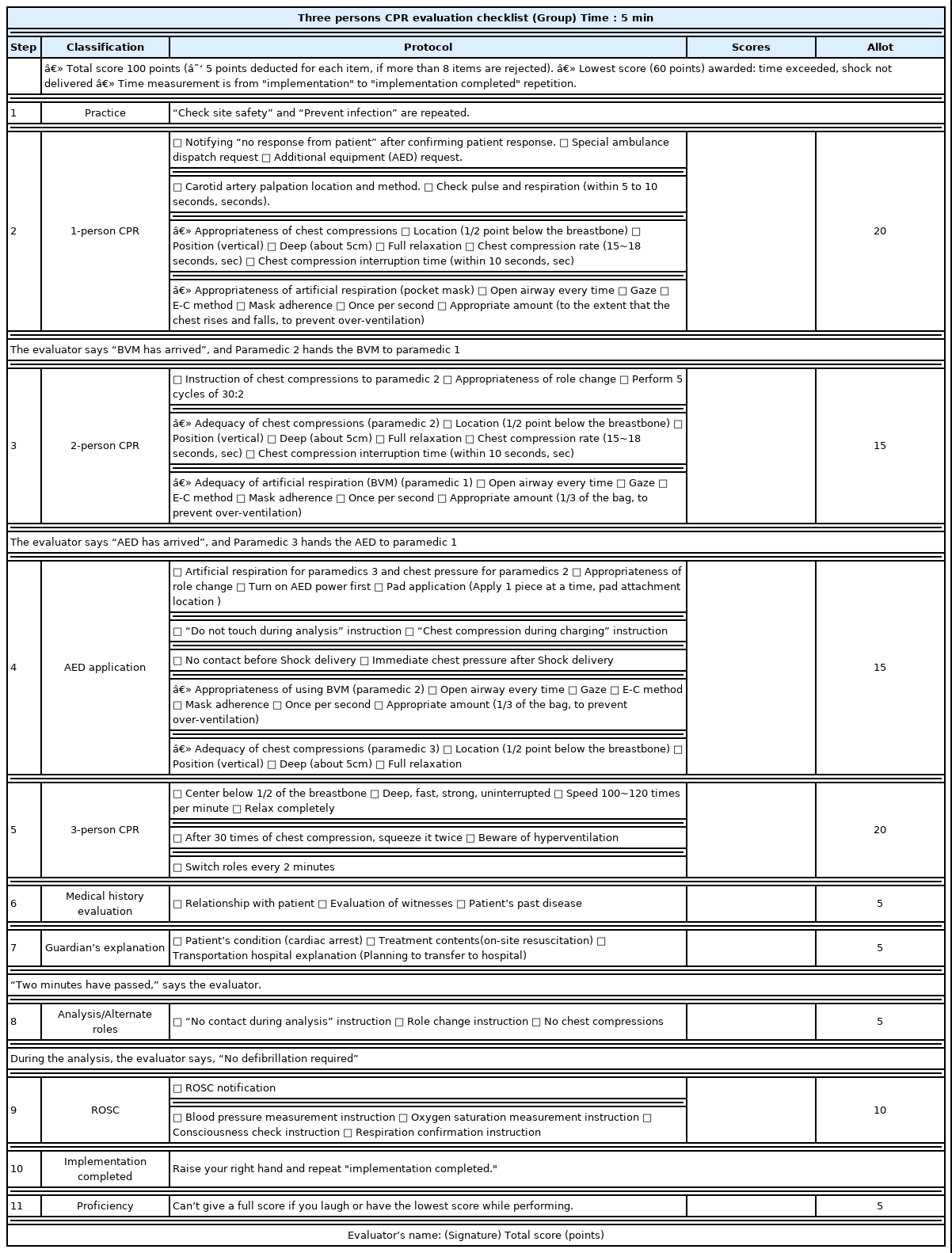
Three persons CPR evaluation
3. 프로토콜 적용을 위한 선행지식
본 프로토콜을 대상자에게 적용하기 위해서는 선행 술기 지식이 필요하다. 이러한 술기 지식에는 1인 CPR(적절한 호흡과 맥박 확인, 가슴압박 적절성, 포켓 마스크 사용), 2인 CPR(적절한 가슴압박과 백밸브마스크[BVM] 적용), 자동제세동기(automated external defibrillator, AED) 사용법, 3인 CPR(적절한 역할 교대), 자발순환회복(return of spontaneous circulation, ROSC) 후 의식 및 호흡 확인, 혈압과 산소포화도 측정 등이다. 이러한 선행 술기 지식은 전문적인 기술을 바탕으로 프로토콜을 적용하고 활용하는데 의의가 있을 것이다.
4. 연구대상 및 프로토콜 구성
본 연구는 소방공무원, 펌뷸런스 대원과 같은 실무자들을 위한 3인 CPR 프로토콜 개발로 응급구조학과 교수, 간호학과 교수, 소방의 구급 지도관을 중심으로 전문가 그룹을 구성하여 프로토콜을 개발하였다. 3인 CPR 프로토콜의 적용 대상자는 현직 소방공무원, 신규 임용된 소방공무원 및 재직자 펌뷸런스 대원을 대상으로 적용할 예정이며, 최소 2인 CPR에 대한 선행지식과 프로토콜을 수행할 수 있는 대상자들이다. 본 프로토콜은 각 11단계로 구성되어 있으며, 각 단계별 수행항목이 도달되는 것을 프로토콜 적용의 최종 원칙으로 한다. 프로토콜 시행 전 평가관의 “환자 발생” 지시와 함께 “실시” 복창하고 실시하며, 의식과 호흡이 없는 성인 환자에게 팀워크를 이루어 소생술을 실시하기 위한 시나리오를 상황에 맞게 제공하는 것을 원칙으로 한다. 또한, 임무 부여는 평가자의 지시에 따라 프로토콜 적용 전 안내한다.
5. 프로토콜 내용 적정성 전문가 평가 및 타당도
본 연구에서 개발된 프로토콜은 2022년 1월15일부터 2월 7일까지 응급구조학과 교수 10인, 간호학과 교수 5인, 현직 소방간부 1인, 총 16인의 전문가에게 의뢰하여 타당도 검증을 받았다. 또한 본 프로토콜은 2020 미국심장협회(AHA)의 가이드라인[4]과 2020 한국심폐소생술 가이드라인[6]을 참고하여 총 11단계로 구성하였으며 각 단계별로 문항별 내용적합도를 구성하였다. 각 문항별 내용 적절성 전문가 평가는 5점 Likert 척도로 ‘매우 적절치 못함’ 0점에서 ‘매우 적절’ 4점으로 측정하며 점수가 높을수록 프로토콜 항목 내용이 적절함을 의미한다. 내용 전문가 평가는 평균과 표준편차를 산출하였으며, 각 문항별 내용 타당도를 평가하기 위해 Lawshe[7]에 의해 제안된 CVR(content validity ratio)을 사용하여 각 문항의 타당도를 확인하였다. 또한, 패널 수가 15명이고 도출된 CVR값이 0.49를 넘는다면 이 문항의 내용타당도를 95% 신뢰도에서 만족한다는 선행연구[8]를 바탕으로 기준점을 제시하였다.
Ⅲ. 연구결과
1. 일반적 특성
본 연구의 일반적 특성을 살펴보면 다음과 같다. 성별은 여자(75%), 나이는 30대(43.8%), 재직 전공 분야는 응급구조(62.4%), 교육 정도는 박사졸업(68.6%), 재직기간은 5년 미만, 5년 이상 10년 미만, 10년 이상 15년 미만, 15년 이상 각각 25%로 나타났다. 시뮬레이션 강의경험은 ‘있다’가 87.5%, CPR 교육 진행 경험은 ‘있다’가 93.8%, CPR 관련 자격증 보유는 ‘있다’가 93.8%로 나타났다<Table 3>.
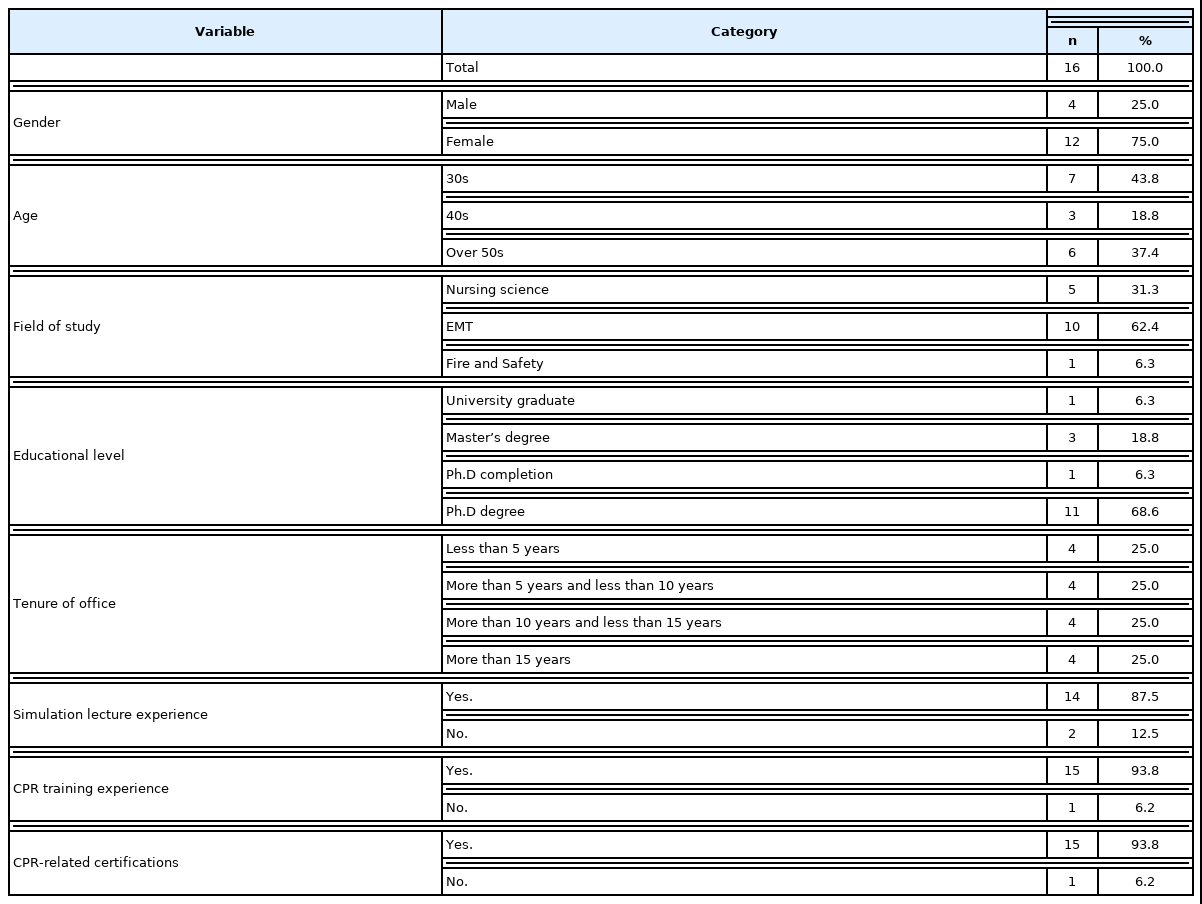
General characteristics of subjects (N=16)
2. CPR 프로토콜 내용 적정성 평가
본 연구의 CPR 프로토콜 내용 적정성 평가를 살펴보면 다음과 같다. 2단계에서는 1인 CPR, 3단계에서는 2인 CPR을 다루고 있으며 총 5개 수행항목에서 평균 3.938~4.000, 표준편차 0.000~0.250, CVR 값은 1.000으로 선행연구 기준값을 충족하였다. 4단계에서는 AED 적용을 다루고 있으며 총 4개 수행항목에서 평균 3.813~3.938, 표준편차 0.250~0.403, CVR 값은 1.000으로 선행연구 기준값을 충족하였다. 5단계에서는 3인 CPR을 다루고 있으며 총 4개 수행항목에서 평균 3.750~3.875, 표준편차 0.500~0.775, CVR 값은 0.875로 선행연구 기준값을 충족하였다. 6단계와 7단계는 병력평가와 보호자 설명을 다루고 있으며 총 2개 수행항목에서 평균 3.750, 표준편차 0.577, CVR 값은 0.875로 선행연구 기준값을 충족하였다. 8단계는 역할교대를 다루고 있으며 총 2개 수행항목에서 평균 3.938, 표준편차 0.250, CVR 값은 1.000으로 선행연구 기준값을 충족하였다. 9단계는 ROSC를 다루고 있으며 총 2개 수행항목에서 평균 3.563~3.625, 표준편차 0.500~0.629, CVR값은 0.875~0.938로 선행연구 기준값을 충족하였다. 마지막으로 11단계는 숙련도를 다루고 있으며, 1개 항목에서 평균 3.375, 표준편차 1.147, CVR값은 0.625로 선행연구 기준값을 충족하였다<Table 4>.

Protocol content adequacy evaluation
Ⅳ. 고 찰
본 연구는 3인 CPR 프로토콜을 개발하고 전문가 집단의 타당도를 검증하여 개발된 프로토콜의 적정성을 평가하는 방법론적 연구이다. 본 연구에서는 검증된 프로토콜을 바탕으로 역할이 구체적이고 명확하게 구분된 3인 심폐소생술을 시행을 통하여 소방공무원을 대상으로 좀 더 심화된 심폐소생술 교육자료를 개발하는데 기초자료를 제공하고자 한다.
본 프로토콜의 경우 기존의 2인에서 3인 CPR로 전환되어 지시자의 역할이 강조되면서 나머지 2명의 역할은 가슴압박, 인공호흡, 그리고 AED 적용에 집중할 수 있게 된다.
본 연구의 3인 CPR에서는 기존의 2인 심폐소생술보다 추가된 인력을 통해 가슴압박, 인공호흡, AED 사용의 유기적인 심폐소생술 적용을 강조하여 좀 더 질 높은 심폐소생술을 제공하고자 한다. 이는 기존에 훈련이나 강의 등에서 실시한 2인 구조법에 활용도가 높아지면서 연속적인 가슴압박과 제세동의 적용을 우선적으로 강조한 나머지 인공호흡이 배제되고 부족한 인원에서 가슴압박과 이송까지 이어져야 하는 악순환의 연속으로 이어졌다[9]. 하지만 선행연구[10]에서 심폐소생술 동안 적절한 기도유지와 환기의 제공은 매우 중요하다고 언급하였는데, 부적절한 환기가 지속될수록 심장의 정상기능 회복에 문제가 생길 수 있고 백-마스크 환기 또는 마스크 밀착에 따른 지속적인 훈련이 고품질 심폐소생술에서 필요하다는 것으로 보아 3인 CPR을 통한 유기적인 가슴압박, 인공호흡, AED 사용의 적용이 계속적으로 필요할 것으로 판단된다. 추후에는 본 프로토콜의 시뮬레이션 적용을 통해 3인 CPR의 유기적인 단계의 연속성을 확보하고 계속적인 훈련과 연구의 보고가 필요할 것이다.
또한 본 연구에서는 3인 CPR을 통해 수행자의 역할 집중도를 강조하였는데 선행연구[11]에서 가슴 압박의 질 저하는 주로 구조자의 피로도 상승을 주요 원인으로 보고 있는데, 반대로 구조의 가슴 압박, 압력과 이완 등의 격려 제공은 가슴압박 정확도와 질에 효과적이라고 하였다[12]. 본 프로토콜에서 제시한 3인 CPR 프로토콜은 제시된 상황에서 각 구조자의 역할을 강조하고, 집중하도록 격려하면서 좀 더 질 높은 심폐소생술의 완성 및 팀웍을 통한 지식과 기술의 공유를 완성하고자 하는데 기여할 것으로 판단된다. 추후 다양한 선행연구의 고찰을 통해 지시자와 역할자의 상호교류가 심폐소생술의 질에 미치는 영향을 다각적으로 검토해 볼 필요가 있을 것이다.
본 프로토콜에서는 보호자에게 환자와의 관계, 과거 질환, 목격 여부를 평가하고 환자의 상태와 처치내용, 이송 예정병원을 설명함으로써 병력평가와 보호자 설명을 추가하였다. 이는 기존 CPR 교육보다 좀 더 현장감과 전문가의 숙련성을 강조하였다. 선행연구[13]에서는 환자의 상태파악과 보호자의 상황인지가 빠를수록 병원 전 단계의 시간 지연을 막고 응급의료서비스 활성화에 기여한다고 하였다. 이는 시뮬레이션을 활용한 구급대원의 표준화된 의사소통을 연구한 선행연구[14]에서도 경력이 적은 대원일수록 현장 업무에 대한 부담감을 많이 느끼는데 교육자와 학습자가 실제 환자 및 보호자와 같은 쌍방향의 의사소통을 적용해 보는 것은 응급 질환 환자 대응에 있어 필수적인 요소로 강조하고 있다. 본 프로토콜에서 적절한 병력평가와 보호자 설명 수행항목의 수행을 통해 추후 소방훈련 등 프로토콜을 실제 적용하는데 있어 현실감을 증가시키고 실제 업무 현장의 이해도를 향상하는데 기여할 수 있을 것이다.
마지막으로 본 3인 CPR 프로토콜에서는 자발순환회복의 영역을 추가하였으며 기존의 2인 심폐소생술 술기의 확장된 영역을 제시하였다. 선행연구[15]에서는 생존퇴원율을 높이기 위해서는 심폐소생술을 포함한 현장에서 환자 상태에 맞는 평가가 적절하게 이루어져야 하고 제세동과 전문심장구조술까지 동반되어야 한다고 하였다. 즉 대상자가 자발순환이 회복되더라도 심정지 증후군 또는 순환부전으로 악영향을 미칠 수 있기 때문에 기존의 2인 CPR의 한계를 넘어 자발순환회복에서의 처치와 기본적인 인지는 필요할 것으로 사료된다[16]. 추후 심폐소생술 술기를 적용할 때도 이러한 부분들을 추가적으로 개선할 필요가 있을 것이다.
본 연구의 제한점은 다음과 같다. 본 연구는 프로토콜의 개발과 전문가 평가를 통해 프로토콜 사용에 대한 적정성을 검증하는 것으로 본 연구에서는 전문가 평가에서 요구하는 기준점을 모두 충족하였다. 하지만 대상자를 선정하여 실제 시뮬레이션 적용을 통해 만족도, 수행 자신감 등 실질적인 변화요인을 측정해 볼 필요가 있을 것이다.
그럼에도 불구하고 본 연구는 3인 CPR 프로토콜 개발을 통해 질 높은 심폐소생술 실시 및 한정된 인원으로 업무의 효율성을 높이고 더 나아가 계속적이고 연속적인 교육과 개정을 통해 응급의료의 만족도를 높이는데 의의가 있다고 본다. 이는 선행연구[17]에서도 심폐소생술에서 생존율을 높이기 위해서는 구급 대원의 수가 최소 3인 이상은 확보되어야 한다는 것으로 보아 본 프로토콜 개발을 통해 실제 현장 업무 중심의 전문화된 프로토콜의 보급으로 질 높고 일원화된 심폐소생술 보급이 필요할 것이다.
Ⅴ. 결 론
본 연구는 3인 CPR 프로토콜을 개발하고 이를 전문가에게 의뢰하여 타당도 검증을 받았다. 개발된 프로토콜은 심정지 환자가 발생한 현장에서 체계화되고 숙련된 CPR 적용하여 그간 2인 CPR의 활용 범위를 넓히고자 한다. 또한, 일선 현장에서 근무하는 소방공무원과 현장에서 생활안전 업무를 담당하고 있는 펌뷸런스 대원 같은 전문가에게 계속적인 CPR 교육 및 인식 개선의 연속성이 확대되어야 할 것이다. 본 프로토콜은 2022년 1월 15일부터 2월 7일까지 응급구조학과 교수 10인, 간호학과 교수 5인, 현직 소방간부 1인, 총 16인의 전문가에게 의뢰하여 타당도 검증을 받았으며, 도출된 최종 CVR 값은 0.625~1.000으로 일반적인 내용 타당도 기준값을 모두 충족하는 것으로 나타났다. 본 연구를 바탕으로 3인 CPR의 품질을 향상시키기 위해 다양한 현장 대상자들을 중심으로 시뮬레이션 검증 및 계속적인 프로토콜 수정이 동반 되어야 할 것이다.