병원 전 응급구조사의 응급분만 프로토콜 개발 및 타당도 검증
The development and validation of a prehospital emergency delivery protocol for paramedics
Article information

Trans Abstract
Purpose:
This study aimed to develop a standardized protocol of systematic and explicit roles and procedures for paramedics for the maternal and newborn management during prehospital emergency delivery situations.
Methods:
This study is a methodological study with detailed step-by-step items proposed by an expert group based on evidence from a literature review. The content validity of the proposed preliminary prehospital emergency delivery protocol was verified before the final protocol was confirmed.
Results:
All 23 detailed items of the preliminary protocol met the reference cut-off (CVI value of 0.8 or higher). After considering, revising, and supplementing expert opinions for each of the 23 items 23 detailed in the proposed protocols, four steps were confirmed. The steps included five items for the management of the imminent mother, 10 items for delivery progress, five items for newborn management, and three items for postpartum management of the mother.
Conclusion:
This study’s findings may serve as reference for developing future specialized training programs for paramedics, to ensure enhanced competence in prehospital emergency delivery situations. The protocol should be reviewed and revised periodically to ensure currency.
Ⅰ. 서 론
1. 연구의 필요성
최근 2년간의 119구급대의 임산부 구급출동 건수를 보면 2021년 1586건, 2022년 2365건으로 점차 늘어나는 추세이며, 구급대원의 도움 속에 구급차 안에서 2021년 63건, 2022년 53건의 응급분만을 시행하였다[1]. 분만을 받는 산부인과가 2010년 808개에서 2020년 517개로 11년간 291개 감소한 것으로 나타났으며[2], 2020년 통계에 따르면 전국 250개 시·군·구 중 산부인과 의료기관이 없거나 산부인과 진료가 가능해도 분만이 어려운 지역이 65개 시·군 구 즉, 전국의 26%에 불가한 것으로 나타나 분만인프라가 붕괴되고 있는 실정이다. 분만취약지역이 증가함에 따라 정부에서는 2011년부터 분만취약지 지원사업을 시행하고 있으며[3], 해당 사업에서 분만이 임박한 상황 발생 시 119를 통해 신속하게 분만의료기관 또는 고위험 산모 처치가 가능한 병원으로 이송되고 있다. 분만실을 갖춘 산부인과 의료기관들이 줄어들고 분만취약지가 늘어나면서 분만 가능한 의료기관 선정에 어려움을 겪고 있어 이송 중 발생하는 응급분만의 필요성이 부각되고 있다[4].
태아의 머리가 자궁에 보이는 배림이 나타나면 즉시 응급분만을 준비해야하고, 산모의 자궁수축이 2~3분 간격임에도 20분내로 분만이 이루어지지 않는다면 신속히 환자를 이송해야 하며[5]. 현장에서의 응급분만의 시간을 놓치면 산모와 태아 모두에게 생명의 위험이 발생할 수 있어 병원 전 응급분만 상황에 대한 응급처치 역량은 필수적이다. 특히 선행연구[6]에서 분만 진통이 산부인과 응급출동 중 가장 많았고 분만 진통이 주호소인 경우에서도 정상분만이 가장 많이 나타났다. 이렇게 응급분만이 이루어지는 현장에 투입되는 119구급대원의 구성은 58%가 응급구조사, 27%가 간호사, 그 외 응급구조사와 간호사의 자격을 모두 갖추고 있으며[1], 총 구성원의 반 이상이 응급구조사로 이루어져 응급구조사의 응급분만 역량 강화와 교육이 필수적이라는 것을 알 수 있다. 119구급대원들의 구급차 내 이송 중 응급분만율은 병원 밖 출생률보다 더 높았으며 그 중 신생아 심정지가 7.3%로 신생아 소생술 및 출산 후 산모관리에 대한 역할 또한 중요해지고 있어, 응급분만에서 발생할 수 있는 돌발상황에 대한 교육 및 업무범위의 확대가 필요하다[4].
그래서 최근 사회에서 응급구조사의 업무범위 조정의 필요성이 인식됨에 따라 24년 만에 응급의료법 시행규칙의 개정으로 2024년도 하반기부터 1급 응급구조사에 한해서 제대결찰 및 절단 등 확대된 업무범위가 시행될 예정이다[7]. 이렇게 병원 전 단계에서 응급분만에 대한 응급구조사의 업무범위 확대는 산모·신생아 관리에 대한 체계적이고 명확한 기준의 프로토콜 및 전문화 교육이 반드시 필요하며, 전문화 교육 이수는 곧 응급분만에 대한 자신감, 만족도, 심리적 안전감 모두 상승되는 결과를 예측할 수 있다[8].
또한 응급분만은 임산부와 더불어 태아의 생명까지 책임져야하는 잠재적인 위험성이 내재되어 있어 더 적극적으로 병원 전 응급처치가 시행되어야 하기에 병원 전 응급분만 프로토콜의 개발은 현장에서 산모와 신생아를 위한 전문적 의료서비스가 반드시 필요하다[9,10].
따라서 본 연구는 병원 전 분만상황에서 응급구조사가 체계적이고 명확한 역할과 절차에 따라 산모와 신생아관리를 수행하는 표준화된 프로토콜을 개발하고자 하며, 더 나아가 본 프로토콜을 통해 병원 전 현장에서 응급구조사의 응급분만 대응역량을 함양시키고 질 높은 산부인과 응급의료체계 교육 프로그램을 개발·운영하는데 기초자료로 제공하고자 한다.
Ⅱ. 연구방법
1. 연구설계
본 연구는 병원 전 분만이 임박한 산모에게 응급구조사가 시행하는 응급분만 프로토콜을 개발하기 위해 문헌고찰을 통한 단계별 세부항목을 작성하고, 이를 근거로 작성된 예비 병원 전 응급분만 프로토콜에 대한 전문가 집단의 내용 타당도를 검증한 후, 최종 병원 전 응급분만 프로토콜을 확정하는 단계를 거치는 방법론적 연구이다.
2. 연구절차
1) 문헌고찰을 통한 예비 프로토콜 항목 도출
본 연구에서는 예비 프로토콜의 항목을 도출하기 위해 Williams Obstetrics 25판, 응급의학 2판, Tintinalli’s Emergency Medicine 8판, 119구급대원 현장응급처치 표준지침, 특수상황전문응급처치학, NREMT PPCP manual을 분석[5, 11-15]하여 응급분만이 임박한 산모관리 5항목, 분만 진행 10항목, 신생아관리 5항목, 분만 후 산모관리 3항목 총 4단계 세부항목 23개를 도출하였다.
2) 전문가 평가를 통한 타당도 검증
예비 프로토콜의 각 단계별 항목에 대한 타당도를 검증하기 위해 2023년 6월 16일부터 6월 23일까지 산부인과 전문의 6인, 응급의학과 전문의 7인, 5년 이상 임상경력의 응급구조사 7인, 총 20인의 전문가에게 의뢰하여 연구 목적을 설명하고 단계별 항목이 나열된 설문지링크를 이메일을 통해 전달하였다. 병원 전 응급분만 프로토콜에 대한 타당도를 확인하기 위해 ‘매우 적절하지 못함’ 1점에서 ‘매우 적절함’ 5점으로 내용 타당도를 측정하였으며 각 항목별 내용에 대해 추가·수정이 필요한 항목에 대하여 의견을 작성하도록 하였다. 각 항목에 대한 타당도를 검증하기 위해 전문가는 평균과 표준편차, 내용 타당도 지수(CVI)값을 사용하여 각 문항의 타당도를 확인하였다. 각 문항에 대한 CVI는 Fehring[16]의 방법을 사용하여 ‘매우 적절하다’ 5(1점), ‘적절하다’ 4(0.75점), ‘보통이다’ 3점(0.5점), ‘적절하지 않다’ 2(0.25점), ‘매우 적절하지 않다’ 1(0점)으로 각 항목에 대한 20명의 전문가가 부여한 가중치의 평균으로 계산하여 CVI값을 산출하여 지수가 0.8 이상인 항목을 선택하였고 추가 의견에 작성된 사항들을 반영하여 수정·보완하였다.
3) 최종 프로토콜 확정
예비 프로토콜에 대한 전문가 타당도 검증 및 전문가 의견을 반영하여 항목을 수정·보완하여 확정된 최종 프로토콜은 응급분만이 필요한 산모관리 5항목, 분만 진행 10항목, 신생아관리 5항목, 분만 후 산모관리 3항목 총 4단계 세부항목 23개로 확정하였다.
Ⅲ. 연구결과
1. 일반적 특성
본 연구의 타당도 검증을 위한 전문가 집단의 일반적 특성을 살펴보면 다음과 같다.
남성 12명(60%), 여성 8명(40%)로 남성이 더 많았으며, 연령은 30대와 50대 이상이 8명(40%)으로 가장 많았다. 재직 전공분야는 응급의학과 전문의와 응급구조사가 7명(35%)으로 동일하게 하였으며, 산부인과 전문의는 6명(30%)으로 나타났다. 교육정도는 석사졸업이 8명(40%)이 가장 많았으며, 박사수료 7명(35%), 박사졸업 3명(15%), 대학졸업 2명(10%)으로 나타났다. 재직기간은 15년 이상이 9명(45%), 5년 이상 10년 미만이 6명(30%), 10년 이상 15년 미만이 5명(25%)으로 나타났다<Table 1>.
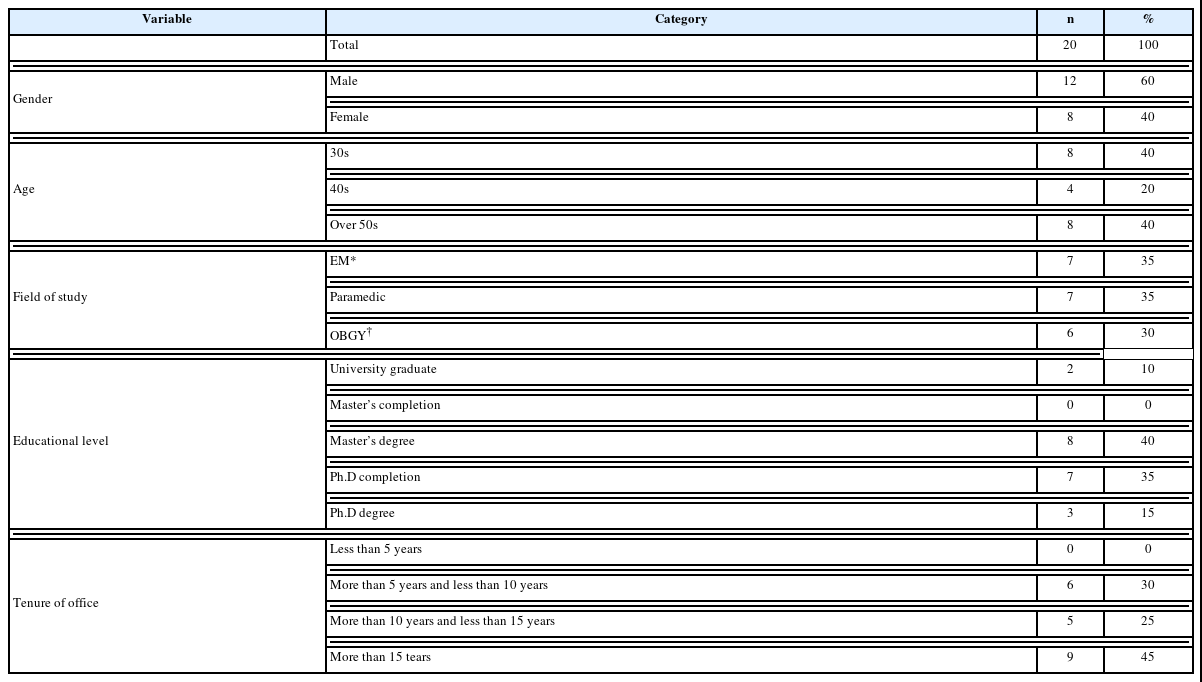
General characteristics of included studies (N=20)
2. 병원 전 응급분만 예비 프로토콜 내용 타당도 검증
본 연구의 병원 전 응급분만 프로토콜 내용 타당도 검증 결과를 살펴보면 다음과 같다.
1단계에서는 출산이 임박한 산모관리를 다루고 있으며, 총 5개 세부항목에서 평균 4.25~5.000, 표준편차 0.000~1.164, CVI값은 0.813~1.000으로 선행연구 기준값을 충족하였다. 2단계에서는 분만진행을 다루고 있으며, 총 10개 세부항목에서 평균 4.500~5.000 표준편차 0.000~0.889, CVI값은 0.875~1.000으로 선행연구 기준값을 충족하였다. 3단계에서는 신생아관리을 다루고 있으며, 총 5개 세부항목에서 평균 4.650~5.000, 표준편차 0.000~0.988, CVR값은 0.913~1.000으로 선행연구 기준값을 충족하였다. 4단계에서는 분만 후 산모관리를 다루고 있으며, 총 3개 세부항목에서 평균 4.600~4.950, 표준편차 0.224~0.681, CVI값은 0.900~0.988 으로 선행연구 기준값을 충족하였다<Table 2>.

Protocol content adequacy evaluation
3. 최종 프로토콜 확정
전문가 타당도 검증을 통해 예비 프로토콜 항목을 수정·보완하여 병원 전 응급분만에 대한 최종 프로토콜을 완성하였다. 예비 프로토콜에서 삭제된 항목은 없었으며 추가된 항목으로는 1단계 분만 전 산모관리 단계에서 산모를 좌측 측와위로 눕히고 임신주수, 분만예정일 통증간격, 임신병력(GPAL)을 확인하는 내용을 추가하였다. 2단계 분만단계에서는 제대가 목에 감겨있는 경우 풀어지지 않으면 제대 결찰 후 절단하여 분만을 진행하도록 내용을 추가하였으며, ‘태아가 양수로 인해 많이 미끄럽다’는 내용과 ‘제대의 소독을 베타딘 또는 헥시딘으로 한다’는 내용으로 수정하였다. ‘태반이 배출될 수 있도록 산모의 배를 시계방향으로 문질러준다’의 항목은 ‘출혈의 가능성과 오히려 태반만출이 지연될 수 있다’는 전문가 의견을 반영하여 ‘태반이 자연스럽게 만출되는지 관찰한다’로 수정하였다. 3단계 신생아 관리단계에서는 신생아에게 자극을 주는 항목에 대해 부드럽게를 삭제하고 ‘신생아의 등이나 발바닥을 문질러 울게 한다’로 수정하였고, 신생아의 의식상태 및 활력징후를 평가하는 시간을 10분에서 5분으로 수정하였다. 4단계 분만 후 산모관리단계에서는 산모의 의식상태 및 활력징후를 5분마다 평가하도록 수정하여 최종 프로토콜을 확정하였다. 따라서 최종 확정된 병원 전 응급분만 프로토콜은 총 4단계 23항목을 확정하였다<Table 3>.
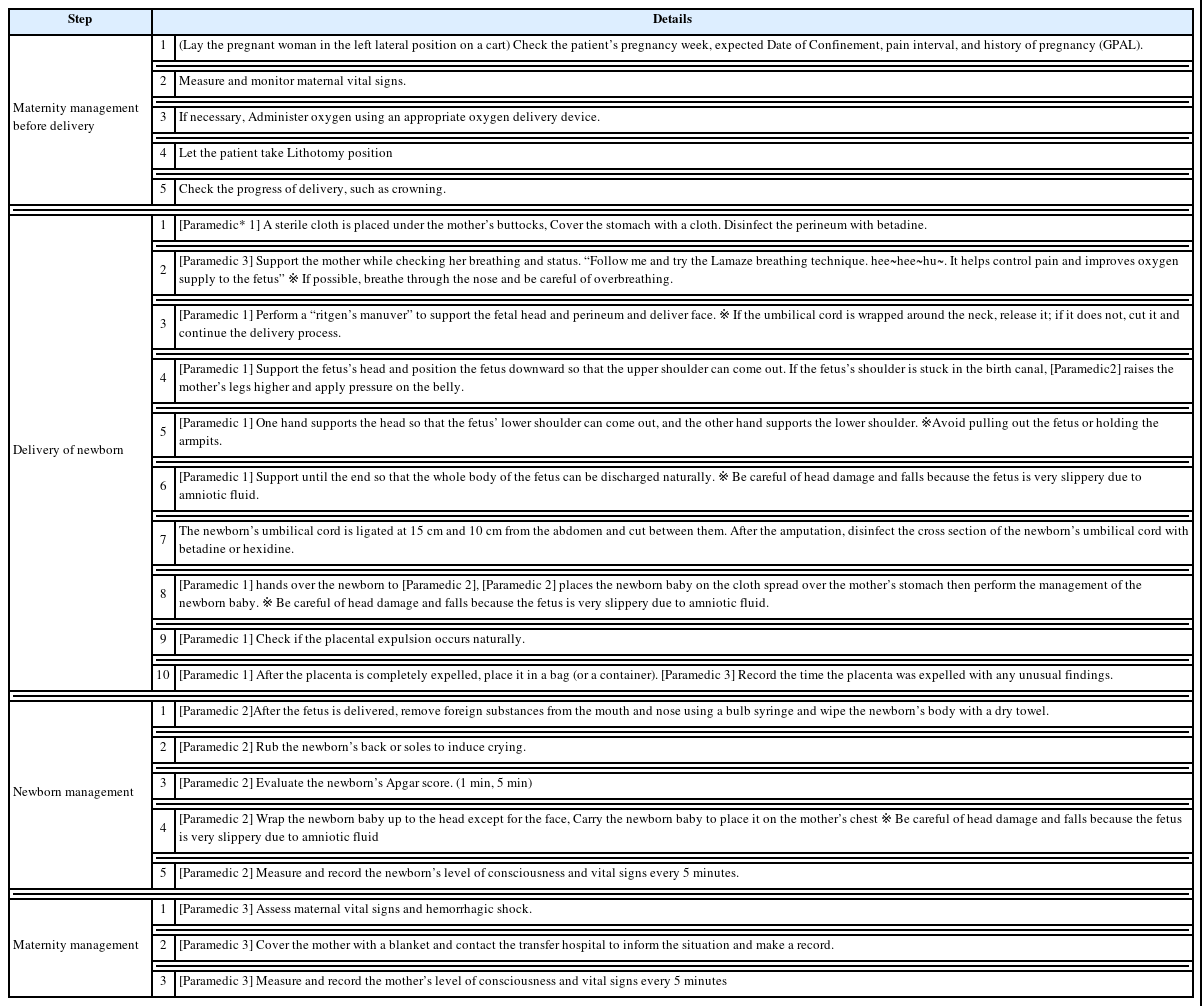
Final Prehospital Emergency delivery protocol
Ⅳ. 고 찰
산부인과 응급상황에서는 산모와 신생아의 생명에 잠재적 위험성이 있어 보다 적극적인 병원 전 응급처치가 시행되어야 하며, 응급구조사들의 응급분만에 대한 역량이 제각기 다를 수 있어 병원 전 산부인과 응급상황에 대한 표준화된 프로토콜의 필요성이 제기되었다[9].
최근 간호사 면허나, 1급 응급구조사 자격을 갖춘 3명의 인원으로 구성된 3인 구급대 탑승이 증가하고[17] 예년에 비해 보다 전문적인 병원 전 처치가 가능함에 따라 체계적이고 양질의 병원 전 응급의료서비스를 제공하기 위하여 현장에서 구급대원 별 역할분담의 중요성이 강조되고 있다. 이로 인해 본 연구는 응급분만이 임박한 상황에서 현장에 있는 응급구조사 3인에게 각각의 역할 부여 및 시행을 위한 프로토콜의 필요성을 인지하고 개발함으로써 개개인의 정확한 역할수행과 원활한 팀워크를 발휘하여, 추후 제한적인 병원 전 환경에서 본 프로토콜을 적용하여 산모 및 태아에게 미치는 영향을 검토해 볼 필요가 있을 것이다.
선행연구[6]에서 자주 접하지 않는 산부인과 환자의 경우 다른 증상을 호소하는 환자에 비해 적절한 환자평가 및 처치가 제공되지 않는다고 나타나 본 프로토콜에서는 산모에 대한 병력평가 항목인 분만예정일, 통증간격, 임신병력 등 산모의 병력청취 항목을 추가하였다. 이는 응급분만이 필요한 상황인지, 다른 산부인과적 응급상황은 아닌지 명확히 구분하는 것이 중요하며 의료지도와 병원선정에 있어 중요한 요인이 될 것이다.
본 프로토콜에서는 병원 전 단계에서 마주하는 응급분만이 필요한 환자는 임신 중후기 이후의 환자들로 하대정맥 압박으로 인한 정맥환류가 떨어질 수 있어[5] 병력을 청취하는 동안에는 좌측 측와위를 취할 수 있도록 하고, 분만을 진행하기 전 준비자세로 Lithotomy 자세를 취할 것을 언급하였다. 또한 자연분만이나 급속분만은 회음부 열상이 발생할 가능성이 있어 회음부 열상을 예방하기 위해 Ritgen’s manuever[18]를 수행하도록 하였으며, 태아의 어깨가 산도에 걸려있는 경우 다리를 더 올리고 복부에 하방으로 압력을 가해주는 술기를 하도록 내용을 구성하였다[19].
신생아에게 제대결찰을 지연시킬 것인지 바로 적용할 것인지에 대해서는 제대결찰을 지연하는 것이 도움이 된다는 연구결과[20]가 있으나 이는 최대 5분을 넘기지 않으며, 2020년 개정된 한국형 심폐소생술 가이드라인[21]에서 신생아가 호흡이 불안정하고 울지 않는 경우, 제대결찰을 지연시키지 않아야 함을 언급하고 있어, 본 프로토콜에서는 병원 전 응급분만 상황에서 제대결찰을 적용할 수 있도록 추가하였다. 또한 제대결찰 및 절단 과정에서 감염의 위험성이 높아지기 때문에 적절한 소독제를 사용하여 소독할 필요가 있는데, 예비 프로토콜에서 작성되었던 알코올이 베타딘과 헥시딘에 비해 피부감염에 덜 효과적이라는 연구결과[22]와 전문가집단의 의견을 반영하여 제대 절단 시 베타딘 또는 헥시딘을 소독제로 사용할 수 있도록 변경하였다. 특히, 분만 시 제대가 목에 감겨있는 상황이 발견될 수 있으며, 제대가 목 주위를 조이는 경우 1분 APGAR 점수가 낮아지고 태아의 고통이 높아지기 때문에[23] 분만 시 제대를 풀어주어야 한다. 하지만 두 번 이상 감겨있는 경우, 어깨를 분만하기 전에 절단하는 것이 도움이 되므로[24] 해당 내용을 추가하여 항목을 구성하였다. 제대결찰 및 절단은 감염관리와 전문적인 술기를 요구하고 있어 교육프로그램에서 응급구조사가 실습해 볼 수 있도록 교육을 구상 할 필요가 있을 것이다.
본 프로토콜에서는 태반이 만출되기 전 자궁 저부를 마사지하면 태반의 분만을 방해하고 출혈을 악화시킬 수 있어[25] 태반이 자연스럽게 배출되는지 관찰하도록 항목을 수정하였다. 또한 전문가 검토 의견에서 태반의 특이점을 파악하고 통에 보관하는 것에 대한 내용타당도가 모두 5점으로 매우 높게 나타났는데, 이는 태반의 크기와 모양, 엽의 개수, 일관성 및 완전성을 파악하는 것이 향후 산모와 신생아에게 발생할 위험요인을 인지하는데 도움이 되기 때문이다[26]. 본 연구에서 개발된 프로토콜에서는 만출된 태반의 특이점을 파악하고 통에 보관한 후 병원으로 이송하여 인계하도록만 언급되어 있어, 향후 교육프로그램에서 태반의 특이점을 파악하는 주제를 다룰 필요가 있을 것으로 사료된다.
프로토콜은 위급한 현장에서 응급환자에 대한 신속하고 정확한 의사결정을 하는데 가이드라인으로써 역할을 하며, 임상 실무에서 활동 중인 구급대원들에게 프로토콜을 바탕으로 한 교육의 만족도가 높다는 연구결과[27]가 있었다. 병원 전 단계에서 예기치 못한 환자 발생에 대비하기 위해 병원 전 응급의료체계에서 근무하는 응급구조사들을 대상으로 보수교육과 전문화 교육이 운영되고 있다. 특히, 실습위주의 시뮬레이션 교육은 가상의 시나리오를 통해 전공지식과 임상수행능력을 향상시킬 수 있는 매우 효과적인 교육방법으로, 실수가 허용되지 않는 임상현장을 대비한 반복연습이 가능하며, 디브리핑에 대한 피드백을 통해 임상에서 적용이 가능하다는 장점을 가지고 있다[28]. 그러나 표준화된 교육과정이 없는 경우 강사의 역량에 따라 교육내용이 일관되지 않을 수 있어[9] 표준화된 프로토콜로 구성된 교육프로그램 개발이 필요할 것이며, 원활한 교육의 진행과 시뮬레이션 교육효과를 증대시키기 위해 강사들을 위한 교육프로그램 또한 개발 및 운영되어야 할 것이다[29].
본 연구는 예비 프로토콜을 제시하고, 전문가 집단의 검토를 통해 최종 프로토콜을 개발하는 연구로, 본 연구에서 개발한 최종 프로토콜을 적용한 교육프로그램을 개발하고 교육함으로써 교육만족도와 응급분만 상황에서의 수행능력 및 자신감 등 실질적인 요인에 미치는 영향을 분석하는 추가연구를 시행하여, 프로토콜의 타당성을 확보해야 할 것으로 사료된다.
본 프로토콜은 병원전 응급분만 상황에서 산모 및 신생아에게 양질의 환자평가 및 응급처치를 수행할 수 있는 역량을 향상시킬 것으로 기대되며, 향후 시뮬레이션 교육과 실제 현장사례 분석을 반영한 프로토콜의 개정과 교육프로그램의 개발이 이루어져야 할 것이다.
Ⅴ. 결 론
본 연구는 병원 전 응급분만 상황에서 응급구조사가 체계적이고 명확한 역할과 절차에 따른 표준화된 프로토콜을 개발하고 이를 전문가에게 의뢰하여 타당도 검증을 받았다.
응급분만 예비 프로토콜은 분만 전 산모관리, 분만 진행, 신생아 관리, 분만 후 산모관리 총 4단계로 구성되었으며 각각의 23개의 세부항목에는 응급분만의 전·후 산모관리와 신생아관리에서 필요한 준비사항과 역할 및 절차에 대해 구체적으로 작성되었다.
본 예비 프로토콜은 2023년 6월 16일부터 6월 23일까지 산부인과 전문의 6인, 응급의학과 전문의 7인, 5년 이상 임상경력의 응급구조사 7인, 총 20인의 전문가에게 의뢰하여 타당도 검증을 받았다. 산출된 CVI값은 선행연구의 기준값을 모두 충족하는 것으로 나타났으며 전문가 의견을 반영하여 수정·보완을 거쳐 최종 프로토콜을 확정하였다.
개발된 프로토콜은 병원 전 분만이 임박한 상황에서 분만 전·후 산모관리와 제대결찰 및 절단을 포함한 신생아관리를 수행하는데 지침이 되고자 하며 응급구조사를 위한 심화된 산과응급 교육프로그램을 개발하는데 기초자료를 제공하고자 한다.
본 연구를 바탕으로 병원 전 단계에서 응급구조사들의 응급분만 대응역량을 함양시키고 질 높은 응급처치를 제공하도록 현장에서 근무하는 응급구조사들을 중심으로 다양한 실습 및 시뮬레이션 교육 프로그램이 개발·운영되어야 하며, 실제 현장사례를 반영하여 지속적인 프로토콜 개정이 동반되어야 할 것이다.