화재진압대원을 위한 심폐소생술 훈련프로그램 개발
Development of cardiopulmonary resuscitation training program for firefighters
Article information

Abstract
연구 목적:
본 연구는 화재 현장에서 발생한 심정지 소방관의 소생률 향상을 위하여 화재진압대원을 위한 심폐소생술 훈련프로그램(FD-CPR)을 개발하고자 하였다.
연구 방법:
행동주의 이론을 전제로 한 FD-CPR 교수설계 모형을 3단계(분석, 설계, 개발) 절차에 따라 개발하였으며, 7명의 전문가 집단(응급의학과 교수 1인, 응급구조학과 교수 1인, 교육학과 교수 1인, 소방학교 교수 2인, 현장 활동 15년 이상 대원 2인)의 내용 타당도 검증(CVI)과 예비 실험을 거쳐 완성하였다.
연구 결과:
7개 절차로 구성된 시나리오 및 16개 항목으로 구성된 수행 능력 평가도구를 개발하였다. 평가도구의 난이도는 평균 41.16%, 변별도는 0.32로 나타나 난이도가 고르며, 변별도가 높은 것으로 확인되었다. 이후, 총 80분짜리 훈련프로그램을 개발하였고, 전문가 7인의 내용 타당도 검증 결과 1.0으로 높았다.
결 론:
본 연구를 통해 국내 처음으로 개발된 화재진압대원을 위한 기본 심폐소생술 훈련프로그램은 화재진압대원들의 심폐소생술 수행 능력 향상에 효과가 있는 것으로 나타났다. 이에 소방학교 신규 화재진압대원 교육과정에 본 프로그램을 넣게 된다면, 심폐소생술에 대한 반복훈련이 이뤄질 수 있으므로 심폐소생술의 수행 능력은 유지될 것이고, 나아가 심정지 동료의 소생률 향상에도 이바지할 수 있을 것으로 기대한다.
Trans Abstract
Purpose:
This study aimed to develop a cardiopulmonary resuscitation training program for firefighters (FD-CPR) to help improve the survival rate after cardiac arrest on the fireground.
Methods:
The FD-CPR was developed following 3 steps of the FD-CPR instructional design based on the behaviorism theory. The content of the program was validated by a group of 7 experts using the contents validity index (CVI) and through a pilot-test.
Results:
A scenario consisting of 7 procedures, and a skill performance evaluation tool consisting of 16 questions were developed. The evaluation tool average score for the difficulty test was 41.16% (even) and that for the discrimination test was 0.32 (high). Subsequently, an 80 min training program was developed. As verified by the 7 experts through the CVI, it was as high as 1.0.
Conclusion:
The FD-CPR developed domestically for the first time in this study was effective in enhancing the CPR performance skills of the firefighters. If FD-CPR is added to the curriculum at the Fire Service Academy educational course for the new firefighters, the CPR performance skills could be maintained. Furthermore, the program can facilitate a better survival rate for colleagues having cardiac arrest on the field.
I. Introduction
1. Necessity
The fireground has multiple risks, such as flames, suffocation, explosion, crash, collapse, burial, and isolation, and only firefighters can usually enter the site. Therefore, if a firefighter suffers from a cardiac arrest on the fireground, only a colleague firefighter is likely to perform CPR, as medical professionals may not be skilled enough to enter the site[1,2].
Cardiopulmonary resuscitation(CPR) is a first aid method to circulate the blood artificially and facilitate breathing when cardiac arrest occurs[3]. When CPR delays a minute, the survival rate decreases 10%[4], but if the witness immediately performs CPR at the site the cardiac arrest occurred, the survival rate can increase by four times, chest compression compared to doing nothing, can even increase the survival rate[5]. The initial electrocardiogram(ECG) mainly showed ventricular fibrillation(VF) or pulseless ventricular tachycardia(Pulseless VT), and defibrillation was inevitable. Every minute of delaying defibrillation decreases the probability of success by 7-10%; on the other hand, defibrillation within a minute after a heart attack may skyrocket the survival rate by 90%[6]. Likewise, the most important factor for the resuscitation of the firefighter suffering from cardiac arrest on the fireground is prompt and precise CPR using automated external defibrillation(AED).
However, the firefighters in the Republic of Korea do not practice CPR at the sites cardiac arrests occur; instead, they move the victim away from the fire scene, despite the time loss, and hand over to paramedics[7]. This may be attributed to the absence of a CPR training program for firefighters. Currently, the 9 Fire Service Academies(FSAs) at the national level have adopted the ‘2015 Korean Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular care,’ which was developed by the Korean Association of Cardiopulmonary Resuscitation(KACPR), for the firefighters waiting for their appointments. This is based on the assumption that the fireground would be safe, the status of the patients would be quickly detectable, and the protective clothing would be easily removed. Visualization is difficult at the fireground, and various noises make it difficult to determine the status of cardiac arrest precisely. Additionally, it is difficult to remove the clothing of colleagues, as it requires a special skill; there are 7 pieces of personal protective equipment consisting of self-contained breathing apparatus(SCBA), personal alert safety system(PASS), protective hood, protective clothing, helmet, gloves, boots. The current KACPR-BLS Program does not consider the characteristics of the foreground, and this limitation has been pointed out to be addressed.
Therefore, firefighters these days prefer the ‘Rescue first, Treatment later’ approach, which prioritizes sending victims away from the fireground and handing them over to paramedics, although it takes longer than immediately performing CPR. This can be attributed to the unique conditions of the fireground, the absence of CPR training, and the restraint of the law. However, the analysis of the reports of the deaths of 33 firefighters on the fireground within the past two decades (from 2000 to 2019) showed that none received CPR at the fireground; all 33 firefighters were moved out from the fireground and handed over to paramedics before they eventually received CPR, which was 38 minutes too late on the average[9].
Based on medical evidence, every 10 minutes of delay in performing CPR reduces the survival rate by 10%. Subsequently practicing ‘Rescue first, treatment later’ does not improve the survival of the firefighters suffering from a cardiac arrest on the fireground. Therefore, the need for an alternative has become pressing, yet there has been no prior study at the domestic level. Accordingly, this study was aimed at developing of the FD-CPR Program to improve the survival rate of firefighters suffering from cardiac arrest on the fireground.
2. Terminology
1) Behaviorism theory
(1) Theoretical definition
The behaviorism theory was developed based on classical conditioning by Pavlov and operant conditioning by Skinner in the early 20th century. It proposes that an action is formed through the repetition and intensification of a stimulus-reaction process; initially, actions are evoked by chance until the designated action can be purposefully evoked[9]. In conclusion, behaviorism states that changes in actions are results of education, and all actions are reactions to the stimulus[10]. This can be more easily applied to actual practice in education because the learning process can be more specific than the insight and exploration suggested by constructivism and cognitivism[11].
(2) Operational definition
The repeated learning that behaviorism emphasizes helps to improve memory, attitude, self-efficacy, and skill performance, among others. Therefore, it can enhance the learning efficiency of CPR[11]. Consequently, to increase the survival rate of firefighters suffering from cardiac arrest, the training should be repeated to allow the firefighters to become habituated to applying a consistent CPR strategy<Fig. 1>.

Behaviorism theory of CPR.
2) ADDIE model for instructional design
(1) Theoretical definition
The ADDIE model for instructional design was one of the models developed during the instructional system development(ISD) for the US army at the University of Florida Education Center(UFEC) in 1975. The ‘Five-step-approach’ from the ISD in the US army manual was revised and called the ADDIE model, using the initials of Analysis, Design, Development, Implementation, and Evaluation[12]. It allows each step to be closely combined with the other step and it is applicable to field operations[13]. It is the most widely used model for developing multiple educational programs, including training on fire safety.
(2) Operational definition
In this study, FD-CPR program was developed by applying 3 steps(analysis, design, development) out of 3 steps of the ADDIE model for instructional design.
3) FD-CPR program
(1) Theoretical definition
The basic CPR training program was introduced by the International Committee on Resuscitation(ILCOR) in 2015 based on the international standard. It is the basic CPR program(KACPR-BLS program) conducted for 80 minutes and targeted at laymen, and it was developed by the Korean Association of Cardiopulmonary Resuscitation[14].
(2) Operational definition
This study is about the FD-CPR program. The program is based on the previous KACPR-BLS program and developed according to the ADDIE instructional design based on the behaviorism theory and in consultation with a group of 7 experts. The training lasts for 80 minutes in total, just like the KACPR-BLS program.
II. Methods
This study consisted of methodological research for developing the FD-CPR program<Table 1>.
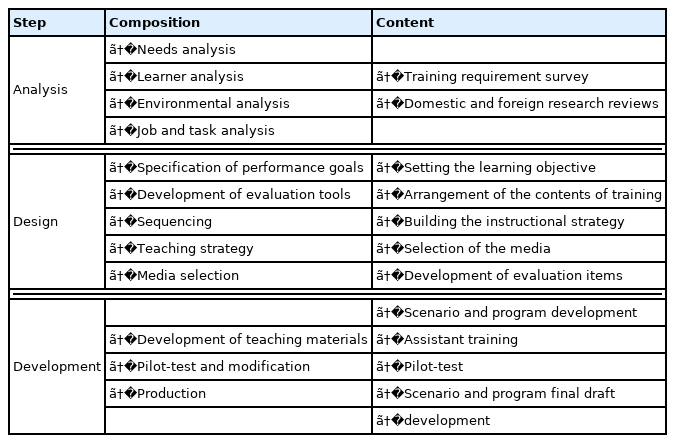
Study design using ADDIE model
1. Step of analysis
The analysis step confirmed the gap between the status of ‘what should be’ and ‘what it is’ before developing the training program, and it provided validity for outcomes of the training [15]. Therefore, it was used to ascertain the need for the program by analyzing prior research through a literature review.
A survey of the need for the training was conducted via intranet with the help of K fire academy, and it involved 200 working firefighters from September 1 to 7. The questions were focused on identifying the problems with performing CPR for firefighters suffering from cardiac arrest at the fireground and providing solutions to them.
Domestic and foreign research reviews were searched from September 1 to 30. For prior domestic research papers related to CPR training for firefighters, I searched the Korean documents from the National Assembly Electronic Library (NANET), Research Information Sharing Service(RISS), Korean-studies Information Service System(KISS), Policy Research Information and Management(PRISM). The foreign papers were obtained from CINAHL, PubMed, SCOPUS, and Google Scholar, among others. The search terms used to filter the previous research papers included ‘firefighter CPR’, ‘CPR training’, ‘CPR education’, ‘CPR program’, ‘Cardiopulmonary resuscitation’, ‘Firefighters & CPR’, ‘CPR & program’, and ‘CPR & training’.
2. Step of design
The design step was used to integrate the results from the analysis step and assess them [15]. Accordingly, I set the learning objective, arranged the contents for training, developed an instructional strategy, selected the media, and developed the evaluation items from October 1 to 30.
Following the suggestion of the group of experts to develop new questions for skill performance to reflect the unique scenarios of the fireground, 16 questions were developed, revised, and supplemented based on the previous appraisal table for the KACPR-BLS Program [16], the main AED textbook for emergency rescue for achieving the second-degree license published by Korea Health Personnel Licensing Examination Institute in 2020[17], Fire tactics I of the main textbooks at the National Fire Service Academy[18], and the test for reacting with the fire by National Fire Service Academy[19]. The contents validity indexes(CVIs) of the developed questions were determined by a group of 6 experts consisting of 1 emergency medicine professor, 1 emergency medical technology professor, 2 fire service academy professors, 1 paramedic, and 1 firefighter with experience of more than 15 years on field. For the points for questions 1-15, 1 point was assigned if the answer was right else 0 was assigned. Higher total points indicated better skill performance. The score for question 16 was estimated based on the time of the initial chest compression; a shorter duration indicated early chest compression.
Additionally, the items of estimating the skill performance were divided into two categories: objective and subjective. Objective estimation involved the use of a Mannequin (the initial chest compression, chest compression spot/depth/speed/pausing time). Subjective estimation was conducted by two evaluators via recorded video (carrying to the safety zone, Securing the supine position, removing the personal protection devices, checking the reaction, asking help, checking the status of breath, chest compression posture, exchanging CPR). To confirm the reliability of the two evaluators based on the intraclass correlation for the subjective estimation, the coefficient (ICC) established by Shrout & Fleiss[21] was applied. According to this standard, ICC was shown as a number from 0 to 1 without a unit of measurement; 1 denoted perfect consistency while 0 denoted no consistency. Generally, a value above 0.75 indicated good consistency[22]. In this study, after 30 sessions of mock examination and calculating the scores and the ICC, a high consistency, denoted by 0.843, was found. In conclusion, the agreement of the two evaluators was high (ICC=0.843, 95 CI= 0.451-0.932, p<.01), and the subjective estimation was conducted.
3. Step of development
The development step involved the production of the materials needed for the program[15]. Therefore, from October 15 to November 13, a group of 7 experts developed the scenario and drafted the training program using the CVI test. They completed the final program after the training of the assistants and the pilot test. Seven experts consisting of 1 emergency medicine professor, 1 emergency medical technology professor, 2 fire service academy professors, 1 education professor, 1 paramedic, and 1 firefighter experienced for more than 15 years on field. Therefore, this program reflected the actual scenarios of the fireground, the medical perspective of CPR, and the educational perspective of training development.
The assistants consisted of 10 members, including 8 instructors at K fire service academy and 2 firefighters at the fire station. All the assistants had experience of more than 10 years with the test for reacting the fire at the second grade or a life-saver license at the second grade. Therefore, they fully understood the fireground and CPR. With these assistants, I proceeded with the overall mock demonstration, prepared for the probable accidents, and specified the task to facilitate the estimation. Specifically, the 8 instructors were divided into 2 groups, with 4 members in each of groups A and B. Each group had 2 persons in charge of the mannequin, and 2 other persons in charge of field safety and recording. The last 2 assistants were in charge of checking the video. They were arranged among the working firefighters at the fire stations because they were not workers of the fire service academy. Consequently, they did not know anything about the participants and the part they were in. All the 10 assistants were given the instructor’s scenario to help them understand, and in case of pilot test, they were assisted to master one step by step with the video.
The pilot test was administered to the 6 firefighters at the actual fire training center of K fire service academy to confirm the overall estimation of the program and its feasibility. The FD-CPR program was developed to utilize the Practice While Watching(PWW) approach to minimize interventions by the instructors and maintain the duration at 80 minutes just as in the control group.
III. Results
1. Step of analysis
1) Training requirement survey
To the question “If a colleague falls on the fireground, will you practice CPR?”, 199 participants out of 200 (99.5%) answered “yes” and 133 (66.8%) preferred the transfer to the nearest safe zone before performing CPR. However, to the question “Are you confident to perform CPR of high quality?”, the answers were mostly “no” (178 participants, 88.0%), and the most common reason was the fear of incompetence related to the lack of a training program (153 participants, 86.0%). To the question about periodic CPR training, the answers were mostly “no” (132 participants, 66%), and the most common reason was the lack of a CPR training program; they added that they did not know how to train for it (100 participants, 75.8%). The 47 participants out of 68 (69.1%) who answered “yes” to the question on practicing CPR answered that they performed CPR on the mannequin just several times and that was all for practicing CPR in a perfunctory way.
In conclusion, the positive attitude of firefighters toward performing CPR would be considered high, but the self-efficacy was low, and because of the absence of a CPR training program, they did not train for it or they performed it ineffectively. The need to develop a CPR training program suited for the actual fireground turned out high (194 participants, 97.0%)<Fig. 2>.
Training requirement survey.
2) Domestic and foreign research reviews
The collected documents from domestic and foreign research were 1,039 in total. Among these, 108 pieces published before 2000 were omitted because they were not satisfactorily related to the study, and 931 pieces were reviewed through a 3-step approach. The first step was to filter out the duplicate documents (n=458) by reviewing the titles. The next step was to omit the irrelevant documents (n=431) by reviewing the abstracts. Finally, 30 documents were chosen after excluding the 12 documents that did not have the statistical data, such as mean and standard deviation, among others, and a mediating variable.
For the domestic documents, there were 6 articles on the development and estimation of the effect of CPR for ordinary people. Among them, there were 3 articles for nurses, and 2 articles for teachers. The articles for firefighters were 3, however they were all for paramedics and none for fire[22]<Table 2>.
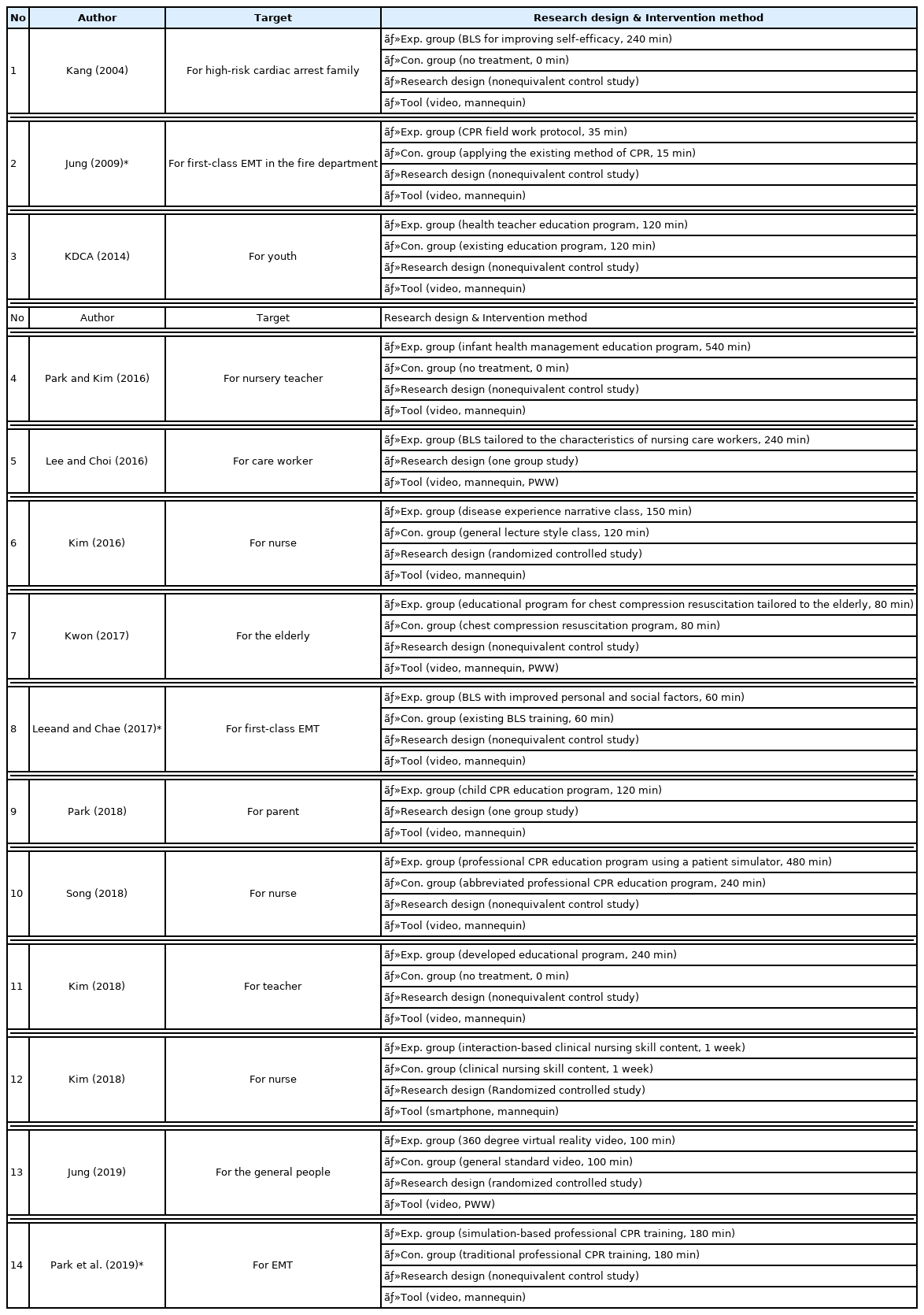
Domestic research reviews
For the foreign documents, there were 16 related to an isolated or fallen firefighter on the fireground, unlike national research. To be more specific, there were 2 research papers on the challenges of the Rapid intervention team(RIT), 1 research paper on the operation of RIT, 3 papers on the apparatus of RIT, and 1 paper on the arrangement of the suburban local RIT. There were 9 papers on the training program for firefighters. Only 3 among these were related to CPR on the fireground[22]<Table 3>.

Foreign research reviews
A review of the 3 documents on CPR for firefighters showed the method by Six Nations Fire & Emergency Services Training Academy in 2017, another method by Herbert & Watford working at Leland Fire Department in 2014, and the last method made by Coral Springs Fire Academy in Florida in the US in 2015 also cited in Kos (2017). However, all of these had not been examined through a hypothesis test, and they only provided suggestions based on the experiences under the local circumstances related to fire.
None of the CPR training programs were tailored to enhancing the survival rate of the firefighters suffering from cardiac arrest. There were ongoing integral studies on the role, apparatus, education, and training of the separately arranged RIT in the foreign countries. However, those were focused on the rapid rescue methods, and the lack of CPR studies applicable to fireground was still existent. There was a limitation related to the structure of the firefighting object, the management of fire officials, the procedure and apparatus of the operations on the fireground; they were different from ours.
2. Step of design
1) Setting the learning objective
The analysis of the training requirement survey and research review of the domestic and foreign documents concluded on the necessity of CPR training program applicable to the actual fireground; the learning objective was set as ‘in the event of cardiac arrest of firefighters at the fireground, high-quality CPR can be provided after moving to a safe zone.’
2) Arrangement of the contents of the training
Based on the learning objective, 7 experts discussed the arrangement of the contents for the training and the instructional strategy. As a result of the discussion, included the 4 essential goals(rapid and precise check of cardiac arrest, prompt report to the station and request for help, high-quality chest compression, and the right use of AED) of the KACPR-BLS program, and some additional methods were recommended to overcome the difficulties on the fireground outlined during the analysis step. Specifically, the added methods included the transfer of the colleague to a safety zone, request for help via radio, application of CPR, removal of private protective apparatus, and the efficient exchange of roles.
3) Building the instructional strategy
To accomplish the learning objective, the following 2 factors were recommended for inclusion in the instructional strategy.
First, focus on learning by practice. The knowledge of CPR is crucial but consistent practice is also important, so the portion of practicing time sets 60 minutes (75.0%) which deems high comparing with the whole percentile.
Second, develop the scenario and program with the actual situation. To enhance the skill performance, focusing on reflecting the scenarios of the fireground was a top priority for the newly developed program.
4) Selection of media
The FD-CPR program adopted the PWW method to prevent distortion of the contents of training and minimize the intervention of the instruct.
5) Development of skill performance evaluation items
It was based on the assessment table for the practice test of the KACPR-BLS program, the assessment table for utilizing the AED for the paramedics for their second-degree license, which was launched at Korea health personnel licensing examination institute, controlling fire tactics I among the main texts at the fire academy, and searching the urgent target required to be saved and rescue among items for assessing the reactive capability against fire. Likewise, the 16 questions were developed and assessed using the difficulty and discrimination test. The average score of the difficulty test was 41.16% (even)<Table 4>. and that for the discrimination test was 0.32 (high)<Table 5>.

Difficulty of skill performance questions
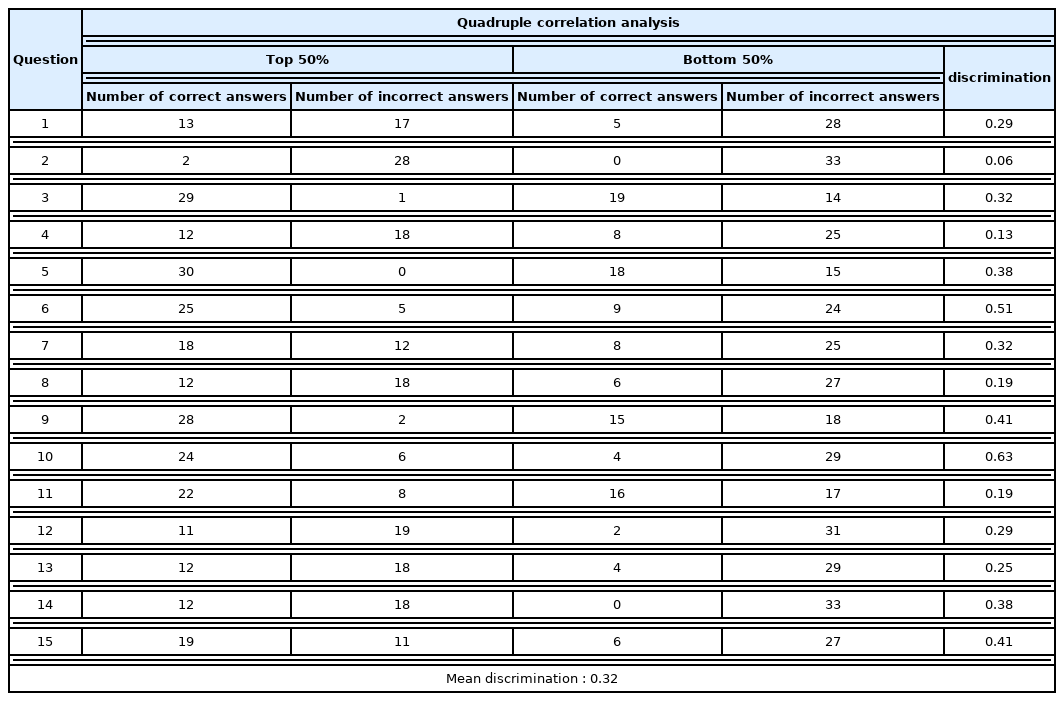
Discrimination of skill performance questions
To secure the CVI of the developed questions, I had it estimated from the group of 6 experts consisting. In this study, the CVI for all the items was estimated as 1.0. However, there were revisions. Question no. 15: ‘Hands-off time’ was revised to ‘time to cease chest compression’ to facilitate its integration with the other appraisal item<Table 6>.

Modification of skill performance No.15
3. Step of development
1) Scenario development
After the discussion by the group of 7 experts consisting of 1 emergency medicine professor, 1 emergency medical technology professor, 2 fire service academy professors, 1 education professor, 1 paramedic, and 1 firefighter, the learning objective, training contents, instructional strategy, selection of the media were decided for developing the scenario for the video for the FD-CPR program. It was divided into 7 steps, and each step was integrated for continuous training.
2) Training program development
Based on the initially developed scenario, the FD-CPR program was developed. The intervention program for the control group It was conducted for 80 minutes just as the KACPR-BLS program. For the training to focus on learning by practice, as emphasized by ILCOR, the practicing time was set to 60 minutes (75.0%), which was considered high<Table 7>.

Development of FD-CPR program
3) Validation of applicability via pilot -test
As a pilot test, the training program was conducted according to the planned procedure, but for the effect on skill performance, there were some problems.
First, too much time passed in checking the status of a fallen colleague on the dark fireground. It is difficult to determine the status of a colleague due to the smoke and impossible to apply CPR due to the flames, collapse, burial, and isolation, among others. Nevertheless, the firefighters tended to report the status of being capable of breath, any symptom of abnormal action, and any traces of trauma precisely, and it rather delayed the performance of CPR.
A revision of step one was made from ‘check the mental status’ of the scenario to ‘check the mental status while tapping the shoulder (“OO chief, are you okay?”)’ as fast and clear yet to act the, accordingly, the related video was altered<Table 8>.

Revising step 1 of scenario
Second, all the methods for carrying colleagues from the fireground to the safety zone varied. In the case of no separate equipment, the methods for carrying were multiple (raise and carrying, crawl forward and carrying, crawl backward and carrying, pull both armpits and carrying, hang on the shoulder and carrying, crawl carrying on the back and carrying, pull the collar and carrying etc.). However, these were for saving the ordinary people on the fireground, and there was no standardized way to save the firefighters wearing personal protective equipment as heavy as 23kg. Therefore, after the discussion of experts, the method of ‘carrying by pulling the collar’ was chosen due to the low possibility of musculoskeletal injury and the ability to move fast. Yet, the firefighter would be wearing the protective clothing and SCBA, and it would be better to apply the ‘drag by pulling the shoulder string’ of the SCBA-frame back carrier rather than the collar of the protective clothing. Additionally, using the shoulder strings with 2 people on a dark fireground would make it difficult to check the precise status of a fallen colleague out of the narrow aisle and cause a delay. Consequently, the roles were specified. Specifically, firefighter 1 would move toward the exit staying down and remove the obstacles in the way and open the exit. Firefighter 2 would carry the fallen colleague by applying the ‘drag by the shoulder string method’ to move to the safety zone out of the exit.
Therefore, step 2 of the scenario, ‘carry to safety zone’ by 2 firefighters was revised to Firefighter 1 should remove the obstacle in the way and open the exit, and the other firefighter should use the method of dragging the shoulder string to carry to the safety zone (5 meters outside the exit). Subsequently, the related video was altered<Table 8>.
Third, because of the protective clothing the firefighters wear, a colleague suffering from cardiac arrest could not be checked properly or receive high-quality CPR. When firefighters wear the mask, fire hood, and helmet, they can hear sounds of their breathlessness loudly, but it also makes it difficult to listen to the breathing sound of a fallen colleague, given the shutting out of external noise and narrowing of the visual field, for abnormal actions to be recognized. The heavy weight of the SCBA interferes with the relaxation of chest compression, and the thick gloves make it difficult to pinpoint the compression position.
Accordingly, step 3 of the scenario for firefighter 1 was modified to add ‘remove the own SCBA and gloves’ before ‘remove the helmet of the fallen colleague;’ that for firefighter 2 was revised to add ‘remove the own SCBA and gloves’ before ‘remove the belts of chest and waist of fallen colleague’. Subsequently, the related video was altered <Table 8>.
Fourth, the quality of CPR depended on the physique of the firefighter. For a fallen colleague wearing SCBA, the victim was over approximately 30cm high. If the physique of the firefighter is small, the posture typically used for chest compression is tilting to one side, which does not keep the arms at right angles. However, raising the knees could keep the arms at right angles and facilitate high- quality CPR.
Step 5 of the scenario was modified: ‘the compressing posture by firefighter 2’ was revised to add ‘alternative 1) kneeling beside the fallen colleague’ and ‘alternative 2) straighten knees beside the fallen colleague’. Accordingly, the related video was altered<Table 8>.
Fifth, the method of pulling both strings of the inner side of the turnout coat and shoulder was not efficient. Pulling both strings of the inner side of the turnout coat and shoulder would cause the unstrung elbow to get caught by the clothing so that it would not be removed. Therefore, it would require several rounds of pulling to remove it, and in the end, it took a long time. Consequently, the pausing time to chest compression would take over 10 seconds, and the survival rate of a colleague would decrease.
Likewise, step 6 of scenario, ‘alternative 1- ready to pull both strings of the inner side of turnout coat and shoulder,’ was removed, and the related video was altered accordingly<Table 8>.
Likewise, the difficulties associated with assessments of the skill performance were all revised to reflect the scenario and video of the intervention program, and this completed the development of the final program<Table 9>. The feasibility of the revised FD-CPR program was tested by the group of 7 experts, and the CVI of all the items was measured as 1.0. therefore, the program was used without further revision<Table 10>.

FD-CPR scenario(after revision)

Content validity index(CVI) of the FD-CPR program
IV. Discussion
According to the statistics of the National Fire Agency (NFA), of the total casualties of 6,193, the dead firefighters accounted for 29 (34.1%) of the most casualties on duty, compared with 9 rescuers (10.6%) and 21 paramedics (24.7%), during the last 15 years from 2005 to 2019. The injured firefighters accounted for 1,376 (22.5%) of the casualties, compared with 575 rescuers (9.4%) and 1,354 paramedics (22.2%). For the US, from 2015 to 2019, 108 (25.9%) out of 417 dead firefighting personnel were firefighters on the fireground, which means that these casualties occur on the fireground[23,24].
Therefore, to enhance the survival rate of firefighters on the fireground, it would be better to apply CPR at the place where cardiac arrest occurred: i.e., a ’Treatment first, Rescue later’ strategy, as opposed to the ’Rescue first, Treatment later’ strategy, as it typically takes a long time to transfer the victim out of the fireground.
However, in the Republic of Korea, there have been studies on CPR to personnel with various occupations, such as doctors, nurses, and teachers. however, there has been no study on firefighters. Abroad, there have been active investigations on the role, apparatus, education, and training of a separately arranged RIT in an integrated manner; however, an RIT could not be organized systematically owing to the lack of firefighters available for field activities. Nevertheless, these studies were focused mostly on the methods of saving the victims and did not investigate the applicable CPR on the fireground. furthermore, the structure of the firefighting object, management of the firefighting personnel, and procedures of operation and apparatus on the fireground, among others, were different from those used here. In the end, a training program appropriate to our situation was developed.
Specifically, a CPR method has been developed based on the behaviorism theory for the theoretical framework to consistently show who the firefighter is according to a group of seven experts, based on the five steps of the ADDIE instructive model, which is widely used in firefighting and safety area training.
The present study had the following strengths. First, to enhance the survival rate of firefighters suffering from cardiac arrest on firegrounds, it was developed focusing on the difficulties brought to light by the training requirement survey and through domestic and international studies. Second, to enhance the applicability of the program, it was developed systematically on the basis of the behaviorism theory for theoretical framework according to 3 steps of the ADDIE model of instructional design. Third, to increase the learning effect of the program, the training focused on learning through practice and that practice time would be 60 min (75%) out of a total of 80 min, which was deemed a high proportion. It was developed as a PWW so that the training contents are not distorted, and it was designed according to the capability and proficiency of the firefighters. Fourth, to help understand the training program, it was distributed after simulating various scenarios for trainees and instructors. Fifth, this is the first-developed CPR program for firefighters through a group consultation of 7 experts. Therefore, it will serve as a standard when developing new FD-CPR programs in the future.
The present study had the following limitations. First, the present study was conducted among firefighters in Gyeonggi-do. Therefore, the potential for extrapolation and generalization for extrapolation and generalization of the study results is limited. Second, the long-term effect of applying the developed training program could not be measured.
V. Conclusion
A scenario consisting of 7 procedures and a skill performance evaluation tool consisting of 16 questions were developed. Evaluation tool is average score of the difficulty test was 41.16%(even) and that for the discrimination test was 0.32(high). After that, a total of 80 min of training program was finally developed, and as a result of verifying the content validity index of 7 experts, it was as high as 1.0(CVI= 1.0).
Hence, the FD-CPR training program developed for the first time in domestic in this study was effective in enhancing the skill performance of the firefighters on CPR. If this program is added to the new firefighters at Fire Service Academy educational course the iterative training to CPR can be conducted, and the skill performance of CPR could be maintained. Furthermore, the program can facilitate a better survival rate fo colleagues suffering from cardiac arrest. In addition, based on the limitations and the results of this study, the following suggestions are recommended.
First, further study regarding the use of the CPR apparatus present currently inside the pump truck and ambulance is necessary.
Second, not only the shortsighted effect of the FD-CPR but also the farsighted effect such as 3 months after and 6 months after to have it estimated requires a follow-up of the study.
Third, when running the RIT afterwards, the firefighters who would have completed this program are suggested to be onboard of the team to enhance the lifesaving performance and CPR skill.